Introduction
Childhood trauma and a previous history of abuse elevate the risk for Dissociative Identity Disorder (DID), Other Specified Dissociative Disorder (OSDD), Depersonalisation/Derealisation Disorder (DDD), Post-Traumatic Stress Disorder Dissociative Type (D-PTSD), and Borderline Personality Disorder (BPD).1–6 A study by Tezcan et al. (2003) found that 100% of patients with dissociative disorders have a history of sexual abuse and other psychiatric co-morbidities.7 The relationship between a history of trauma or abuse and dissociative disorders has been reported in the literature.8,9
Dissociative disorders include DID, DDD, and dissociative amnesia (DA). The Diagnostic and Statistical Manual of Mental Disorders 5 (DSM-V) defines DID, formerly multiple personality disorder, as having 2 or more distinct personalities, recurrent gaps in memory, and alterations in affect, behaviour, consciousness, perception, cognition, and/or sensory or motor function.10 DID has a lifetime prevalence of 1.5%.11 Patients are diagnosed with OSDD if they do not meet the full criteria for DID, DDD, or DA. OSDD is defined similarly to DID but with unclear identities or absence of amnesia.12 OSDD also includes dissociative disorder with specific symptoms, such as an acute dissociative reaction. One study reported an OSDD prevalence rate of 8.3%.12 Depersonalisation is the persistent feeling of detachment from oneself, and derealisation is the subjective sense of detachment from reality or living in a “dream-like” state.13 DDD has a prevalence of 1% in the general population.8
Other psychiatric disorders associated with dissociative features or increased co-morbidity with dissociative disorders are D-PTSD, and BPD, a type of personality disorder. D-PTSD is defined by symptoms of PTSD with depersonalisation and/or derealisation, cognitive impairment, hypnotisable state, and amnesia.15 D-PTSD has a prevalence of 12 to 15% in all PTSD patients.9,14 The DSM-V definition of BPD includes an inability to maintain long-term relationships, increased sensitivity to rejection, unstable self-identity, and impulsivity.15 BPD is prevalent in 1.6% of the general population.15 Therefore, our patient’s previous diagnoses of PTSD and BPD may be contributing to her current presentation as well as to the differential diagnosis.
This case study describes a 22-year-old woman with a significant history of physical abuse, sexual assault, and numerous medical and psychiatric comorbidities. She initially came to the hospital with suicidal thoughts and a specific plan, later showing symptoms suggestive of DID, OSDD, DDD, BPD, and/or a display of regression, a defence mechanism. The case delves into a possible diagnosis given her unique symptoms consisting of the coexistence of her seven identities, her true self and six alters, each with unique experiences and memories, and her ability to switch between them: all rare features of dissociative disorders.
Because DID has been historically misdiagnosed or inaccurately treated, patients reporting multiple identities must be evaluated thoroughly and accurately.16,17 An interesting finding that can help in the diagnosis is that the patient could switch between identities and remember the events of each alter. In an event of childhood sexual trauma, like in our patient, victims may experience dissociation, an immature coping mechanism where a person unconsciously disconnects from reality due to stressors that result in impairment of memory, perception, and sense of self.18
Patient Information
The patient is a 22-year-old female with a psychiatric history of Major Depressive Disorder, Post-Traumatic Stress Disorder (PTSD), Generalised Anxiety Disorder, suicidal ideation, BPD, Anorexia Nervosa, and Tourette’s. The patient’s medical history is significant for Hypothyroidism, Postural Orthostatic Tachycardia Syndrome (POTS), Scoliosis which required spinal fusion, Irritable Bowel Syndrome, Diverticulitis, and Fibromyalgia. The patient presented to the hospital because of suicidal ideation with plans to cut herself. The patient was adopted and previously lived a high-functioning life as a clothing store employee. The patient did not report any significant family, medical, or psychiatric history. The patient reports a history of physical abuse and sexual assault that led to an unplanned pregnancy, which resulted in miscarriage. The patient did not explicitly share the exact dates of traumatic events. The patient shared that her history of physical abuse and sexual assault triggers her suicidal ideations. Previous treatments including fluoxetine, escitalopram, aripiprazole, brexpiprazole, quetiapine, desvenlafaxine, sertraline, and electroconvulsive therapy proved ineffective.
Clinical Findings
The patient initially presented to the hospital due to having an active plan to hurt herself. The patient reported obsessions around self-harm and alignment, which led to compulsions executed around hurting herself, such as head banging and strangulation. The patient reported that she struggled with expressing her feelings and explained that her repression of emotions led to thoughts of hurting herself. She also wrote down her thoughts in her journal, which mainly dealt with themes of guilt, sadness, violation of personal space, powerlessness, and inability to express her emotions due to social constraints.
The patient also exhibited traits of BPD, an existing diagnosis, during her hospital stay. A diagnosis of BPD can be made if a patient presents with five of the nine following symptoms: (1) frantic efforts to avoid real or imagined abandonment, (2) pattern of unstable and intense interpersonal relationships characterized by alternating between extremes of idealization and devaluation, (3) identity disturbance: markedly and persistently unstable self-image or sense of self, (4) impulsivity in at least two areas that are potentially self-damaging, (5) recurrent suicidal behaviour, gestures, or threats, or self-mutilating behaviour, (6) affective instability due to a marked reactivity of mood, (7) chronic feelings of emptiness, (8) inappropriate, intense anger or difficulty controlling anger, (9) transient, stress-related paranoid ideation or severe dissociative symptoms. All of which the patient exhibited or reported during her hospital stay. For example, during patient interviews, the patient displayed splitting towards her parents and healthcare providers at the hospital. The patient also displayed sensitivity to rejection or criticism as she became distraught and executed actions of self-harm when another patient called her “fat.”
The patient was also treated for an existing diagnosis of PTSD. A diagnosis of PTSD can be made if a patient presents with at least one symptom in each criterion: A, B, C, and D. Criterion A is met when exposed to actual or threatened death, serious injury, or sexual violence through direct experience, witnessing, or learning about it happening to a close family member or friend, with an emphasis on violent or accidental incidents or repeated exposure to aversive details. Criterion B involves intrusion symptoms post-traumatic event, including distressing memories, dreams, dissociative reactions, and intense psychological or physiological distress triggered by cues resembling the traumatic event. Criterion C is marked by persistent avoidance of stimuli associated with the event, demonstrated through efforts to avoid distressing memories, thoughts, or external reminders. Criterion D indicates negative alterations in cognitions and mood after the event, such as inability to remember a key aspect due to DA or persistent negative beliefs about oneself, others, or the world. Criterion E is trauma-related alterations in arousal and reactivity that began or worsened after the traumatic event(s), as evidenced by two (or more) of the following: Irritable behaviour and angry outbursts, reckless or self-destructive behaviour, hypervigilance, exaggerated startle response, problems with concentration, sleep disturbance. The patient met DSM-V criteria for PTSD because she directly experienced repeated physical, sexual, and emotional abuse at a young age (Criterion A), experiences recurrent “flashbacks from the rape” and distressing dreams related to the traumatic events (Criterion B), exhibits efforts to avoid distressing memories, thoughts, or feelings about or closely associated with the traumatic events (Criterion C), experiences dissociative symptoms (Criterion D), holds persistent and exaggerated negative beliefs or expectations about oneself, others, or the world (Criterion D), has anger outbursts (Criterion D), demonstrates self-destructive behaviour through self-harm (Criterion D), problems with concentration (Criterion D), and has trouble falling asleep (Criterion D).
The patient shared the identities of her six “alters” other than her true self who are all different ages. “Alter A” is 3 to 5 years old, “Alter B” is 6 years old, “Alter C” is 10 years old, “Alter D” is 17 years old, “Alter E” is 18 years old, and “Alter F” is “ageless.” The attending physician met with “Alter C” and “Alter E” during the patient’s hospital stay. The patient could switch between alters by acknowledging that one alter would like to step forward and speak. She reported that she switches every 2 hours to one day. However, she can get “stuck” with one alter for up to 5 days. The patient can remember the events happening to each alter and reports that the alters know each other’s existence.
“Alter C” is a ten-year-old female with selective mutism. During the psychiatric evaluation, “Alter C” spoke in a baby-like voice but was able to use medical terms proficiently. She used colours to describe feelings or neologisms in communication. For example, brown meant comfort, blue meant sad, red meant angry, and “angie” also meant angry. She reported that she was sexually abused and experiences an increase in self-harm compulsions because the alter does not know how to express her feelings and cope appropriately.
“Alter E” is an 18-year-old female with appropriate language and coping skills and does not report desires to self-harm. During the psychiatric evaluation, she described herself as the “grown-up” who protects the “littles,” the younger alters. “Alter E” says she shares the responsibility with the patient’s true self. She reports feeling very tired from taking care of the alters and of her efforts in quieting the younger alters. She also reports difficulty with concentration because the alters are talking to one another. “Alter E” describes the experience as a “merry-go-round” where the alters know what is going on and take turns coming forward. Throughout the patient’s 26-day stay in the hospital, the attending physician spoke with “Alter C” multiple times and “Alter E” once.
Timeline
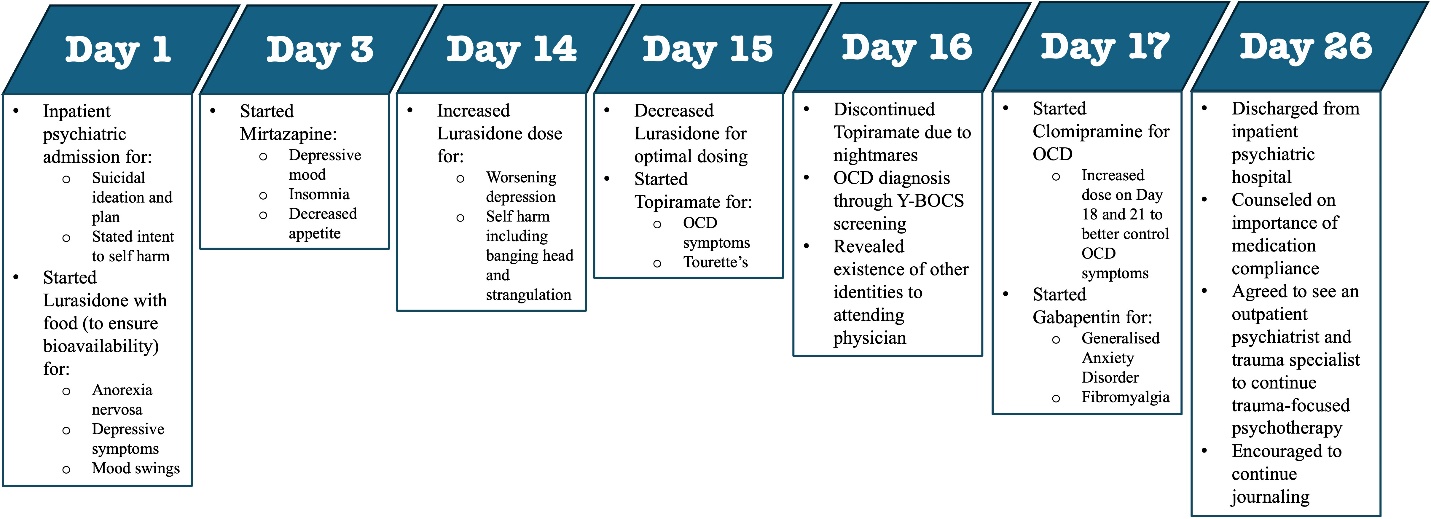
The patient was seen with previously reported symptoms throughout her 26-day hospital stay. See Figure 1 for a timeline of the patient’s 26-day hospital course. The patient initially met criteria for inpatient psychiatric admission due to her suicidal thoughts, active suicide plan, and stated intent to hurt herself. Previous treatments (fluoxetine, escitalopram, aripiprazole, brexpiprazole, quetiapine, desvenlafaxine, sertraline, and electroconvulsive therapy) in outside hospitals were reported to be ineffective in improving the patient’s mood. The new medications, clomipramine, lurasidone, mirtazapine, and gabapentin, as well as journaling and counselling, worked well in alleviating the patient’s mood and anxiety symptoms. The patient’s suicidal thoughts, depressive thoughts, anxiety, obsessions, and compulsions gradually decreased over the 26-day course. The patient’s inpatient care team counselled the patient on the importance of medication compliance and outpatient follow-up, and the patient agreed to see an outpatient psychiatrist and trauma specialist to continue trauma-focused psychotherapy.

Diagnostic Assessment
The patient met the criteria for inpatient admission because she was actively suicidal and had plans for self-harm. Pertinent laboratory tests were drawn, and all were within normal limits.
The patient exhibited obsessions and compulsions around self-harm, leading to the diagnosis of OCD. The patient’s Yale–Brown Obsessive–Compulsive Scale (YBOCS) total score was 29 with an obsession subtotal of 17 and a compulsion subtotal of 12. See Table 1 for Children’s YBOCS ancillary dimension score breakdown.
The patient exhibited all nine of the DSM-V criteria mentioned above for BPD, supporting the patient’s existing diagnosis of BPD. The patient also met all DSM-V criteria for PTSD, supporting the patient’s existing diagnosis of PTSD.
OSDD is a diagnosis of exclusion, so there are no specific DSM-V criteria for OSDD. Patients are diagnosed with OSDD if they do not meet criteria for DID, DDD, or DA. DID is the presence of two or more distinct identities or personality states, along with recurrent gaps in memory and significant distress or impairment. DDD is defined as recurrent experiences of depersonalisation and/or derealisation that cause significant distress or impairment to daily functioning. DA is the inability to recall important autobiographical information, typically related to traumatic or stressful events, that is inconsistent with ordinary forgetfulness, which causes significant distress or impairment. The patient does not fit criteria for DID or DA because she does not experience recurrent gaps in memory. The patient’s presentation does not fit DDD as she put more emphasis on her 7 identities rather than feeling detached from herself or her surroundings.
Therapeutic Intervention
The patient’s final medication list was as follows: clomipramine 150 milligrams every evening for OCD and mood, lurasidone 60 milligrams every day with food to ensure bioavailability for mood, mirtazapine 15 milligrams every evening for mood, insomnia, and appetite stimulation, clonidine 0.2 milligrams every evening for nightmares and POTS, fludrocortisone 0.1 milligrams every evening for POTS, gabapentin 300 milligrams three times a day for Generalised Anxiety Disorder and fibromyalgia, and levothyroxine 88 micrograms every day for hypothyroidism. The patient was compliant with all medications.
The patient was provided with various psychosocial interventions, including daily rounds (meeting with the entire psychiatric team including the attending physician, residents, and medical students), activities in the milieu (leisure activities such as watching movies and colouring with other patients), nursing education groups (educational sessions on emotional regulation and coping strategies), and case management (working with the social worker for housing and community resources upon discharge). The patient was continuously encouraged to express herself through therapy and journaling. The patient continued to endorse multiple identities therapeutically managed by the attending physician with counselling and education on new and existing psychiatric diagnoses and treatment methods. At the end of the 26-day hospital course, the patient endorsed ability to better control mood swings and compulsions for self-harm, improved depressed mood, and no active suicide ideations, which were her initial indications for admission.
Follow-up and Outcomes
There is no current medication or therapeutic guidelines exist for OSDD, except for cognitive behavioural therapy, both in the United States and internationally. Because of the patient’s extensive history of trauma and unique presentation of dissociative symptoms, trauma-focused psychotherapy was recommended as opposed to untargeted therapy.19 Trauma-focused psychotherapy for OSDD requires long-term commitment. Therefore, treatment for OSDD was to be initiated and continued in an outpatient setting due to the patient’s fear of the concept of identity integration and the time constraint imposed by the inpatient setting. The patient was counselled on the importance of long-term trauma-focused psychotherapy with a trauma specialist due to the debilitating effects multiple identities can have on the patient’s daily life. The patient was also counselled to call an emergency line or return to a psychiatric hospital if her obsessions and compulsions around self-harm become unmanageable or if she becomes actively suicidal again.
Discussion
A 22-year-old woman, with a notable background of physical abuse and sexual assault, was initially hospitalized due to suicidal intentions. Throughout her hospital stay, two of the patient’s six alternate identities were observed. The patient disclosed experiencing all seven identities simultaneously, retaining memories of each alter’s events, and switching between identities.
This case study was complex and had a broad differential diagnosis including DID, OSDD due to trauma, DDD, D-PTSD, BPD, and/or regression as a defence mechanism (Table 2). An interesting finding that can help in the diagnosis is that the patient could switch identities and remember each alter’s events. In an event of childhood sexual trauma, like in the case of our patient, victims may experience dissociation, a maladaptive coping mechanism where a person unconsciously disconnects from reality due to environmental or personal stressors that result in impairment of memory, perception, and sense of self.17 The trauma model of dissociation supports the relationship between trauma and dissociation. For example, one study reported patients who experienced dissociation in their cohort reported a history of trauma.17 Therefore, the presence of alters in our patients could be a manifestation of dissociation.
Patients seeking treatment for DID have historically been misdiagnosed or received inaccurate treatment and spend years seeking treatment before being correctly diagnosed due to social stigma and the complex nature of the disorder.17,18 Because DID has been historically misdiagnosed, patients reporting multiple identities must be evaluated thoroughly and accurately. DA is often experienced in patients with DID.20 For example, van Minnen & Tibben reported a case in 2021 of a patient who developed multiple identities after being sexually abused.21 In the earlier case, the patient reported finding toys and girls’ clothing in her home without knowing she bought them and experienced lapses in her memory. A similarity between this patient and our patient is that both reported being preoccupied with organizing or negotiating with the identities in their heads. There is, however, a reported case of a patient who can switch between identities in a short period, enough to switch during fMRI studies.22 Our patient’s ability to switch between alters does not seem to be utterly voluntary as she describes feelings of being “stuck” as one alter for more extended periods. A diagnosis of OSDD may be appropriate for our patient as she reports the presence of alters but no symptoms of amnesia.
Mild depersonalisation and derealisation can be experienced in the non-pathological population in the setting of sleep deprivation and substance abuse.23 Pathologic depersonalisation and derealisation disrupt daily functioning. Salgado et al. reported a patient describing derealisation as being hollow or in someone else’s body.24 In contrast, our patient did not describe physical feelings of detachment from her body or reality when describing seeing her alters in a “merry-go-round” and living in parallel. Moreover, our patient described her experience as 7 identities co-existing in time with separate dialogues and traits. Our patient has a previous psychiatric diagnosis of PTSD, so her alters could be manifestations of the dissociative aspects of D-PTSD, a subtype of PTSD. However, like DDD, patients diagnosed with D-PTSD experience feelings of detachment from themselves or reality rather than assuming multiple identities.
Like DID, OSDD, DDD, and D-PTSD, studies have found that childhood sexual abuse, like in our patient’s case, is a significant risk factor for BPD.5,25 A study by Krause-Utz reported that up to 80% of BPD patients experience dissociative symptoms, such as depersonalisation and derealisation, and that the severity of dissociative symptoms correlated with the severity of past trauma.26 Identity disturbance, part of the criteria for a diagnosis in BPD, encompasses four factors: role absorption (being absorbed by one role), painful incoherence (patient’s subjective distress due to incoherence), inconsistency (observed incoherence), and lack of commitment (unable to commit to jobs or values).23,25,27 Identity switching in our patient is evidence of a lack of commitment to identity. Our patient also exhibits signs of painful incoherence and inconsistency because “Alter E” reports distress while managing her alters and the attending physician observed the patient switch between alters during patient interviews, respectively. Therefore, a combination of the patient’s history of severe childhood sexual assault and identity disturbance in BPD may have contributed to the formation of alters in our patient.28
Children and adolescents exhibit various methods of coping with stress and trauma, such as regression. Regression is an immature defence mechanism where the person reverts to an earlier stage in development.29,30 Regression is expected in the paediatric population and addressing the underlying cause resolves the regression.30 However, regression can present in the adult population when one is triggered by trauma or stress.29,30 The presence of “Alter C” could be episodes of regression the patient experiences when triggered by memories of the patient’s history of physical and sexual abuse. In 1995, Jacobsen et al. reported a case study of a patient with selective mutism that manifested due to the different identities preventing the patient from speaking to ensure information about past trauma would not be shared.31 “Alter C’s” selective mutism could be like the aforementioned case study as our patient may be pressured not to share specific information on past trauma or sexual abuse. In 2022, O’Donovan et al. reported a case study of a 12-year-old patient with PTSD, anxiety, and depression presenting with suicidal ideations who voluntarily entered a “headspace” of a 6-year-old, which served as a learned coping mechanism for her childhood trauma.29 This maladaptive voluntary regression was learned through social media. The case mentioned above is like our patient in that the patient shows signs of regression as “Alter C” however, it is unclear if our patient’s regression is genuinely voluntary.
Given high co-morbidities in psychiatric disorders, especially dissociative disorders, PTSD, and BPD, making a definitive diagnosis for this patient is deemed problematic.27 The patient’s symptoms do not align with a diagnosis of DID or DDD as she is aware of all of her alters and can intermittently switch between alters. Furthermore, the patient displayed splitting, dissociation, and regression, all maladaptive coping mechanisms. Integrating the patient’s history of childhood trauma and sexual assault, previous diagnoses of PTSD and BPD, and symptoms of dissociation with the presence of alters, our patient’s experience may be due to OSDD and pathologic defence mechanisms of dissociation and regression due to history of previous childhood trauma. Limitations of this case report include small sample size (n=1) and lack of complete generalizability. Strengths lie in describing a unique case that can help other providers who encounter such a rare phenomenon and be able to help differentiate between the diagnosis.
Patient Perspective
The patient initially endorsed fear when sharing her multiple identities. She reported that the integration of the alters was a scary concept for the patient because of the loss of the alters. The alters also reported feeling scared to come forward but longed to trust in the process of getting exposed. The patient shared her identities and had the identities “come forward” to reveal themselves after spending time and establishing trust with the attending physician. The patient thought she had OSDD and, therefore, agreed with the diagnosis. She shared that she could express herself through journaling and conversation. She was made aware of the long-term commitment required for OSDD. The patient agreed to follow up with a trauma specialist after discharge to continue counselling and therapy for her new diagnosis of OSDD.
Conclusion
Overall, this was a complex case of a 22-year-old female, with a notable history of physical abuse and sexual assault, who was diagnosed with OCD, displayed BPD traits, and disclosed the existence of six other identities in addition to her true self during her hospitalization. As the attending physician met with two of the six alternate identities, the patient revealed that she was experiencing all seven identities simultaneously and could intermittently switch between the alters. In this study, we explored a wide range of potential diagnoses. The patient’s distinctive ability to intermittently switch between the alters combined with the fact that there is a high prevalence of comorbidities in psychiatric disorders, especially dissociative disorders, PTSD, and BPD, arriving at a definitive diagnosis was challenging. Moreover, she displayed behaviours like splitting, dissociation, and regression, which are regarded as maladaptive ego-defensive mechanisms. Given our patient’s extensive history of trauma, previous psychiatric diagnoses, and current dissociative presentation, we conclude that a diagnosis of OSDD and pathologic defence mechanisms of dissociation and regression may be appropriate.
This case represents the complexity of diagnosing dissociative symptoms in the context of extensive childhood physical, sexual, and emotional trauma. Childhood trauma is a risk factor for many psychiatric illnesses, such as depression, suicidal ideation, DID, OSDD, DDD, D-PTSD, and BPD. This highlights the various negative manifestations previous trauma has on one’s well-being, even in previously high-functioning people. Because DID has been historically misdiagnosed, this case report presents the challenges in making a definitive dissociative diagnosis, especially in the context where significant childhood trauma can lead to many symptoms, therefore blurring the lines between different diagnoses.
Ethical Considerations
The patient signed a paper consent form indicating that her case would be discussed in academic journals after removing any identifying information. Case reports do not require institutional review board approval at our institution, and in the United States of America as a whole.32 This case report adhered to the Clinical Research and Ethics Committee’s regulations and the Helsinki Declaration of the World Medical Association.
Disclosures
All authors have no conflicts of interest to disclose.
Funding Source Declaration
All authors have not received any financial support for the research, authorship and/or publication of the article.
Author Contributions
All authors have approved the manuscript and agree with its submission to the International Journal of Psychiatric Trainees.
Acknowledgements
Authors did not declare any acknowledgements.