Background
Suicide remains a major global public health concern, with more than 700,000 individuals dying by suicide globally each year. The World Health Organisation therefore recommends four evidence-based interventions in suicide prevention, with one of them being interaction with media for responsible reporting of suicide.1 There are a wide range of risk factors influencing suicide and suicidal behaviour. Demographic factors include living in low and middle-income countries, age, and gender, with men being twice as likely to die from suicide. Socioeconomic factors such as low income, limited education, urbanisation, inadequate housing, and broader issues like climate change, war, and forced migration also contribute significantly to suicide risk. Groups including LGBTQ+ individuals, residents of high-security psychiatric hospitals, first responders, and people living with chronic physical or mental illness are also at increased risk. A personal history of suicide attempts is a predictor of suicide risk and suicidal behaviour.2,3
Stigma surrounding suicide, as with mental illness more broadly, is highly prevalent, with the consequences of stigma to both suicide and towards mental health disorders being risk factors themselves for suicidality.4,5 The consequences of stigma may be detrimental to those who have attempted suicide and those close to them, further isolating these individuals.6,7 Thus, stigma is a deterrent to help-seeking and help provision in both individuals experiencing suicidal ideation and those supporting them, both from professionals and informally.8
Integral to countering stigma is the use of appropriate and sensitive language when talking about suicide. Sensitive language in suicide is mostly discussed in media reporting of suicide, where several guidelines have been issued throughout the years. The World Health Organisation guidelines and Samaritans Guidelines have highlighted the importance of responsible reporting using respectful, accurate and non-judgmental language.9,10
Discharge summaries are a critical part of patient care. They are not only a handover of the events occurring during a hospital admission, but also contain critical information which is required to be handed over to other care providers and relatives to ensure adequate continuity of care. High-quality discharge summaries have the potential to avoid adverse patient outcomes.11 Discharge letters documenting past suicide attempts can be used to inform risk assessment.
Suicide attempts should always be documented in a patient’s discharge summary, as this is a critical component for future risk assessments and crisis management planning. Discharge summaries are vital to patient care, providing invaluable information to outpatient and emergency services. However, they are also accessible to the patient and their loved ones. Suicide attempts often evoke a range of challenging emotions in those affected, including shame, guilt, and feelings of failure.12,13 For this reason, these incidents must be recorded with the utmost sensitivity and respect.
Stigma, both public and perceived, is associated with an increased risk of suicidal thoughts and behaviours in those with a history of suicide attempts, those who have been bereaved by suicide and even the general public. Individuals with a history of suicide attempts report greater fear of being judged for their history of suicidality. Stigma may evoke secrecy surrounding suicidal behaviours, and anticipated stigma in itself may become a barrier to help-seeking in the future. These effects may lead to social withdrawal and isolation, which in themselves are risk factors for suicide.14
Given these dynamics, it is crucial for clinicians to be guided by evidence-based frameworks that promote non-stigmatising communication. The International Association for Suicide Prevention (IASP) Language Guidelines offer practical recommendations for appropriate terminology, emphasising the use of language that is neutral, respectful, and person-centred.15
This audit was conducted at the public inpatient mental health hospital in Malta. In the local healthcare system, hospitals operate using a firm-based model that comprises foundation year doctors (newly graduated doctors who have not yet obtained their full medical warrant), specialist trainees, specialists, and consultants. Within this structure, the responsibility for drafting discharge summaries typically falls on foundation year doctors. These discharge summaries serve as key clinical documents and include essential information such as patient demographics, diagnoses, clinical course, treatment upon discharge, and follow-up arrangements.
This audit aimed to assess the quality of documentation of suicide attempts and suicidal behaviour in psychiatric discharge summaries, with a specific focus on adherence to the IASP Language Guidelines. By evaluating current practices, this audit seeks to highlight opportunities for improving clinical communication and reducing stigma within mental healthcare settings.
Methods
Ethical Approval
Ethical approval was not required as per local hospital policy since no patient contact was sought. Data protection approval was obtained from the relevant individuals, and all data was processed and stored in accordance with GDPR regulations.
Setting
This paper describes a clinical audit carried out at Mount Carmel Hospital, Malta between January 2023 and July 2024. Mount Carmel Hospital is the country’s only psychiatric hospital, offering inpatient care to patients with a range of mental health conditions.
Inclusion and Exclusion Criteria
The discharge summaries of all admissions between January and July 2023 and January and July 2024, written by foundation doctors, were screened according to the inclusion criteria. Patients of all ages who had a suicide attempt or suicide-related behaviour surrounding admission were included in the study. Suicidality or suicidal behaviour did not necessarily need to be the primary reason for admission. There were no inclusion or exclusion criteria based on discharge diagnosis.
They were excluded if no discharge letter was available or if there was no evidence of suicidality or suicidal behaviour in the discharge letter. Patients with multiple suicide attempts within the data collection were included more than once. However, each discharge summary was considered as a stand-alone entry.
Audit Cycles
This audit was divided into two cycles. In the first cycle, the discharge summaries of all patients admitted between 23rd January and 30th July 2023 were screened retrospectively. This corresponds to the third (Q3) and fourth (Q4) quarter of 2023 for foundation year doctors.
In the second cycle, the discharge summaries of all patients admitted between 29th January and 27th July 2024 were screened retrospectively as per the same inclusion criteria. This corresponds to the third (Q3) and fourth (Q4) quarter of 2024 for foundation year doctors.
Standard
Each discharge letter included in the study was reviewed by individual authors, each of whom was responsible for evaluating a subset of the discharge summaries meeting the established inclusion criteria. Each discharge letter was assessed independently. If doubt was present, the discharge summary would be flagged and reviewed by two other reviewers.
If a discharge letter contained multiple errors each error was classified separately. This approach allowed for a detailed breakdown of the errors present in the discharge summaries and provided a clearer view of common or recurring problems.
In both cycles, the discharge letters were assessed for their adherence to IASP’s language guidelines.15 Namely, they were reviewed for use of stigmatising language such as ‘commit suicide’ and ‘failed suicide’, as well as amount of detail when documenting an attempt. Excessive detail was defined as detail which is not necessary for the clinical management of the patient. Table 1 below summarises the IASP language guidelines.
Intervention
The authors gave a short presentation to foundation year doctors during their psychiatry rotation induction talk. This was done twice for two separate groups of doctors, once in January 2024 and once in July 2024. The presentation consisted of a 10-minute talk and Microsoft Power Point presentation, highlighting the importance of using sensitive language when it comes to discharge summaries and discussing the implications of stigmatising or graphic language on both other healthcare professionals and patients. The IASP guidelines were shared amongst the doctors.9 The authors also presented examples and led a discussion regarding more appropriate phrases that can be used in discharge letters. The presentation slides were distributed amongst the foundation doctors after the talk.
Statistical Analysis
Descriptive and inferential statistical analysis was conducted using Microsoft Excel to compare results of the first and second cycle. Inferential analysis consisted of the independent sample t-test and the Chi squared test.
Results
First Cycle
A total of 1393 patients were admitted between January and July 2023. Of these, 503 were excluded as no discharge letter was available (36%). Of the remaining 890, 24% fit the inclusion criteria (n = 215). Of the included individuals, 59.5% were males (n = 128), whereas 40.5% were females (n = 87). The mean age of those included was 38. The youngest was 12 years old while the oldest was 85 years old.
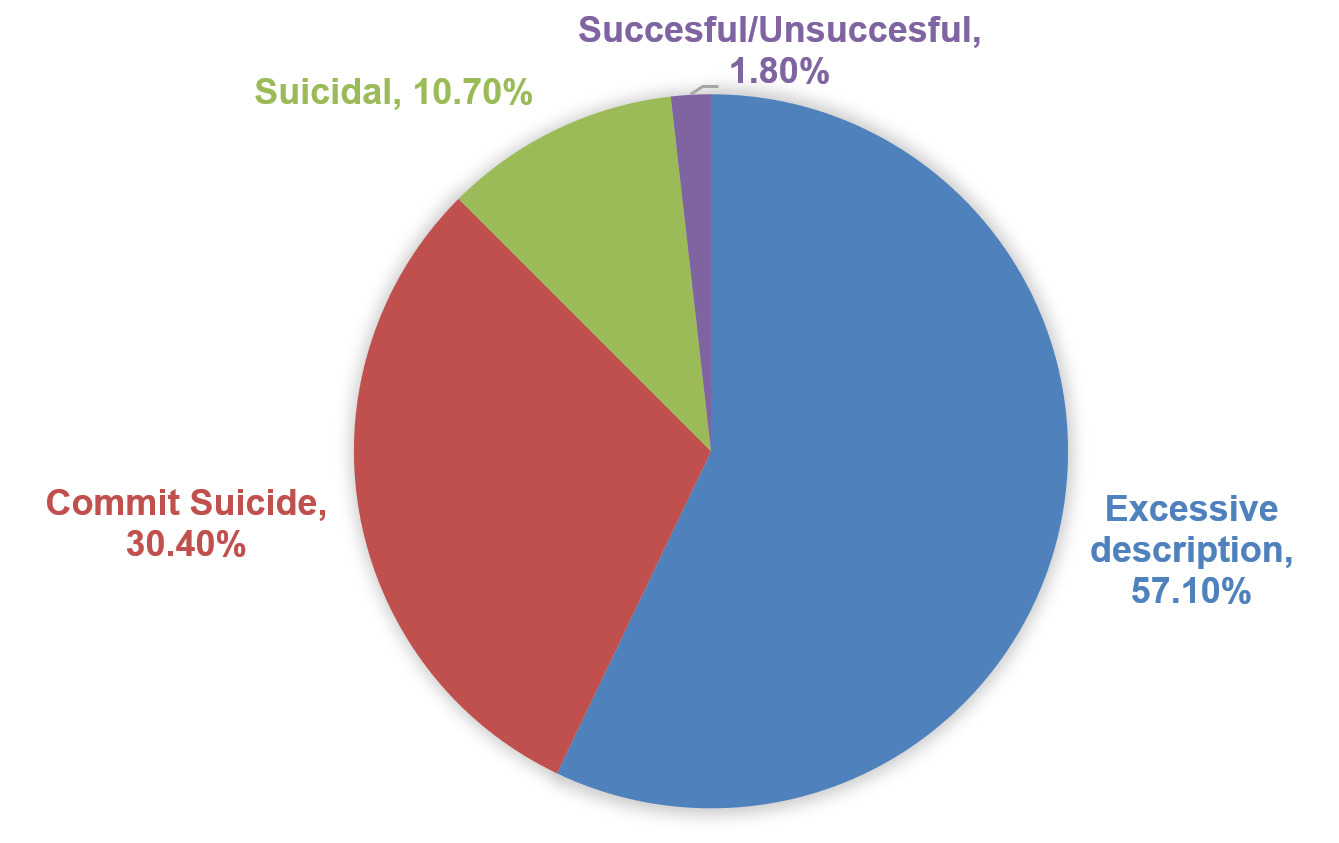
26% of discharge letters did not use appropriate suicide-related terminology (n = 56). Of these, the most common issues were with excessive description of the attempt (53%) and use of the phrase ‘commit suicide’ (28%). There was no statistically significant difference in the amount of discharges containing errors between adults and minors (𝜒 = 0.046, p = 0.830). The distribution of errors can be seen in Figure 1.
.png)
Second Cycle
A total of 1335 patients were admitted between January and July 2024. Of these, 332 were excluded as no discharge letter was available (25%). Of the remaining 1003, 13% fit the inclusion criteria (n = 171). Of those included, 49.7% were males (n = 85) and 50.3% were females (n = 86). The mean age of those included was 34. The youngest was 11 years old and the oldest 77 years old.
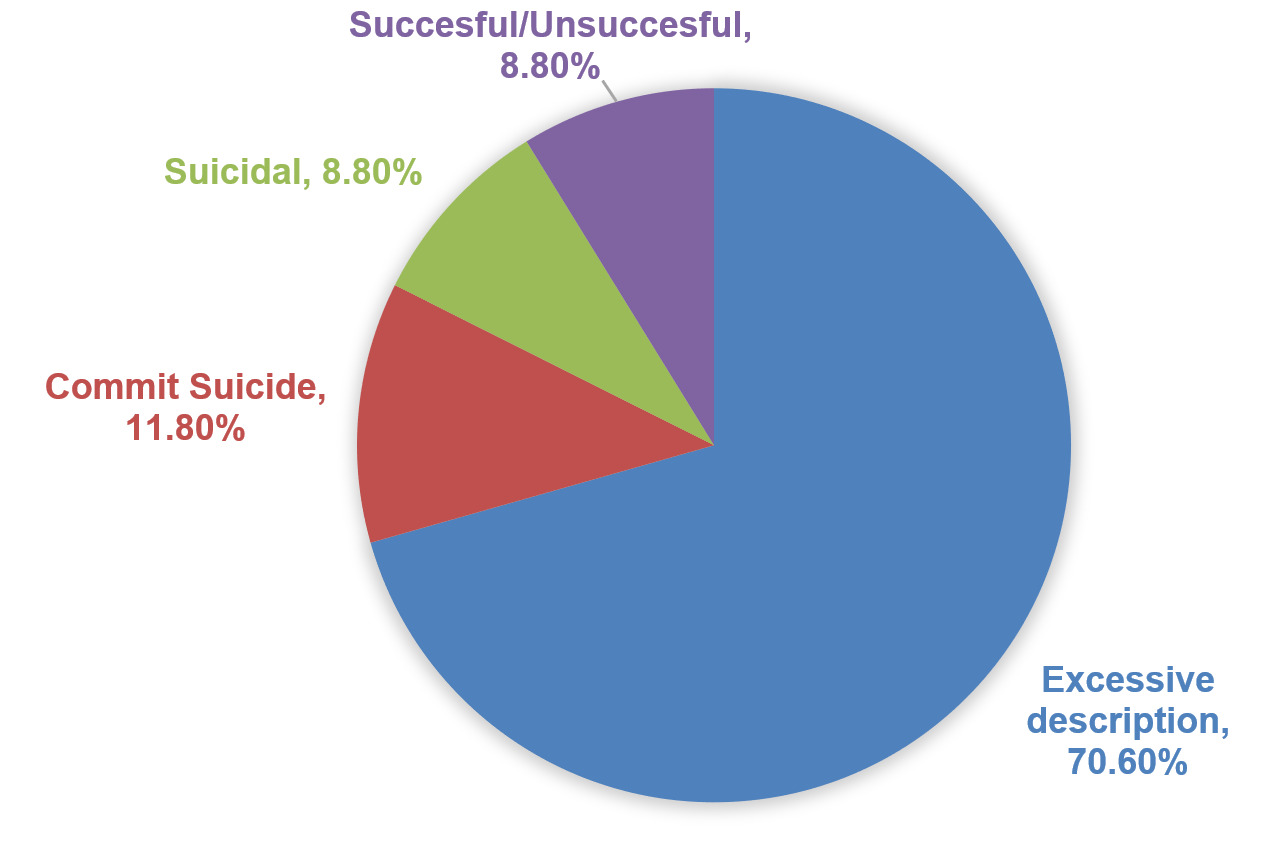
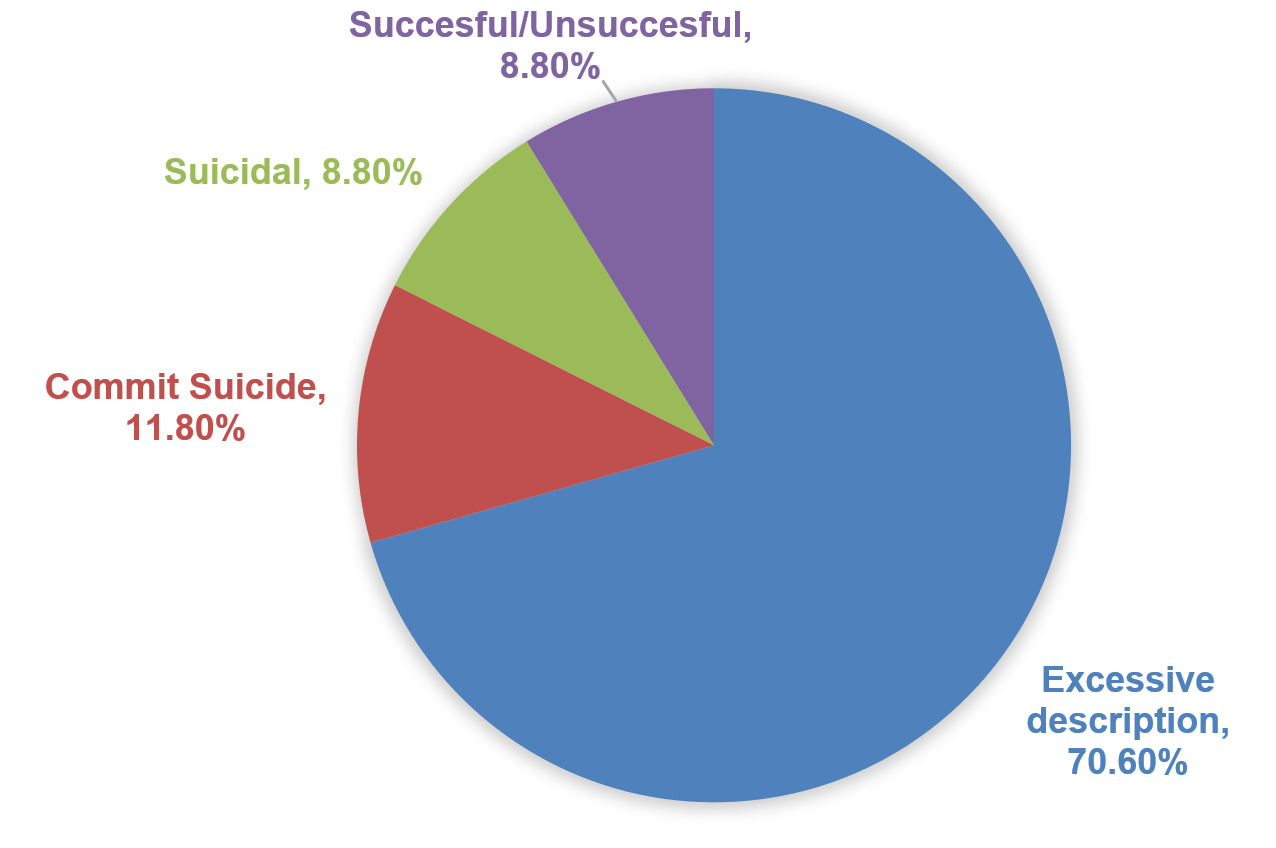
20% of discharges did not use appropriate suicide-related terminology (n = 34). There was no statistically significant difference in the amount of discharges containing errors between adults and minors (𝜒 = 0.164, p = 0.686). The most common issue was excessive description of the attempt (70%). The distribution of errors can be seen in Figure 2.
Comparing Audit Cycles
Table 2 shows the sex and age characteristics of the included patients in the first and second cycle.
Between the first and the second audit cycle there was a 6% decrease in the number of discharge letters that did not comply with IASP’s language guidelines. The intervention significantly reduced the use of the phrase ‘commit suicide’ (OR 0.279; CI 0.092 to 0.845, p = 0.024). Table 3 shows the percentage of discharges containing the respective error out of the total number of eligible discharges.
Discussion
Interpretation of findings
Given the well-established association of stigma as a barrier to help-seeking and contributing to an increased suicide risk, every point of contact should prioritise non-stigmatising practices, in particular in written documentation that may be accessed by patients or their families.16
The audit’s findings show a measurable improvement in the quality of suicide related documentation in patients’ discharge summaries. Prior to the intervention, a quarter of discharge summaries did not adhere to the IASP’s language guidelines. This means that one out of every four individuals admitted on a background of suicidal behaviour were given a discharge letter that was potentially graphic, insensitive or stigmatising in nature. This decreased to 20% or one out of every five individuals after the intervention. Of note, the use of the phrase ‘commit suicide’ decreased significantly as a result of the intervention. This is of particular importance due to the criminalising connotations associated with the term commit when used in association with suicide, which contributes to the stigma surrounding suicide.17 This emphasises the importance of familiarisation and adherence to evidence-based guidelines, such as those provided by the IASP, when communicating about suicide. Despite the existing guidelines being targeted towards media professionals, this audit emphasises that they are also applicable to clinical settings.
Appropriate communication about suicide has shown to have the ability to decrease suicidal ideation.18 This fortifies our recommendation to include suicide sensitive language training in medical education. This is particularly important given that medical students may hold negative attitudes towards those presenting with suicidal behaviour.19 Foundation year doctors may find suicide uncomfortable to discuss suicide and struggle with appropriate documentation of suicide. These results are promising, especially given that the intervention is neither time-consuming nor costly. This indicates that a short session in which foundation year doctors are made aware of the issue and guided on how to write about suicide appropriately can not only improve the quality of patient care but also reduce iatrogenic harm. This is not only beneficial for documentation purposes but also for general communication about suicide with patients and their relatives.
Foundation doctors should be taught how to write sensitive discharge letters and how to discuss suicide during their psychiatry induction talk. Ideally, this talk is given to all foundation trainees, not only ones in psychiatry, as all of them will come across patients affected by suicide at some point in their practice. Additionally, foundation doctors should be supported and supervised by more senior firm members to ensure that discharge letters are not only of good quality but also written sensitively and sensibly.
These findings support the growing body of research that emphasises the impact language can have on mental health outcomes.20 Stigmatising language may not only reinforce public misconceptions but also increase internalised stigma in vulnerable patients, which in turn may result in lower self-esteem and treatment adherence, and even increase the risk of suicide. Furthermore, clinical documentation is an influential communication tool which is seen by multiple professionals and patients themselves. Insensitive language may damage the therapeutic alliance as well as have adverse psychological effects on the patient and those close to them.21
Limitations
The main limitation for this audit is the subjective quality of the ‘excessive description’ criteria, where it was left up to the discretion of the data collectors to decide whether this applied. This was mitigated by having the same researchers collect the data for both the first and the second cycle to minimise bias. Furthermore, it was noted that in the second cycle, errors were repeatedly made by the same individuals. This could have negatively skewed the results since such individuals had authored a large proportion of discharges. This implies the actual impact of the intervention may have been greater than reported. In addition to the above, the discharge diagnosis was not collected during the data collection period. Moreover, further information regarding method of attempted suicide, number of previous attempts and comorbid substance use were not collected. Future research to involve these data points may provide more in-depth insights into this cohort of patients. Furthermore, this research was performed in a single country and a single institution, and this thus limits its generalizability. Lastly, while immediate improvements in language use are measured, long term retention of sensitivity training could not be assessed.
Conclusion
This audit provides unique insights into the situation in Malta. However, findings remain relevant to healthcare systems in general due to challenges faced with respect to stigma and lack of training in the communication of suicide in medical curricula. The audit provides preliminary evidence showing that simple and targeted interventions can yield significant improvement in the quality and sensitivity of documentation through the alignment with guidelines such as the IASP.
AUTHORS’ CONTRIBUTIONS
Conceptualization was conducted by Dr. Nicole Borg and Dr Rachel Gambin; Methodology was developed by Dr. Nicole Borg, Dr. Rachel Gambin and Dr. Gianluca Gatt; Investigation and data curation were carried out by Dr. Nicole Borg, Dr. Rachel Gambin and Dr Gianluca Gatt; Formal analysis was conducted by Dr. Nicole Borg; Writing of the original draft was handled by Dr. Nicole Borg, with review and editing by Dr. Rachel Gambin, Dr. Gianluca Gatt, and Dr. Fabrizia Cassar; Supervision was provided by Dr. Fabrizia Cassar; and project administration was overseen by Dr. Nicole Borg. All authors contributed significantly to the research and preparation of the article, and read and approved the final version before publication.
ETHICS STATEMENT
This study followed the ethical standards of the 2013 Helsinki declaration and its later amendments or comparable ethical standards. Ethical approval was not required as per local hospital policy since no patient contact was sought. Data protection approval was obtained from the relevant individuals, and all data was processed and stored in accordance with GDPR regulations.
DECLARATION OF CONFLICT OF INTEREST
The authors declare that they have no conflicts of interest, financial or otherwise.
ROLE OF FUNDING
No funding was received for conducting this study.