INTRODUCTION
The thalamus acts as a relay for the bidirectional flow of information between cortical and subcortical regions and different cortical areas. It plays a significant role in transmitting and regulating sensory input, and thalamic lesions often present with multimodal sensory abnormalities.1
Several studies have reported the importance of the thalamus, particularly the pulvinar, anterior, and dorsomedial nuclei, as the substrate for information-processing anomalies in patients with schizophrenia. These appear to be related to a reduction of thalamic volume relative to total brain size, and functional imaging studies show reduced structural connectivity between the thalamus and prefrontal and cingulate cortices.1,2
CASE
A sixty-seven-year-old right-handed woman presented to the emergency department with a 3-week history of behavioural abnormalities. She exhibited persecutory ideas involving her husband and medical staff, along with decision-making difficulties and doubts regarding autobiographical events in the week before admission. Her medical history included dyslipidaemia, with no history of alcohol or drug abuse and no personal or family history of psychiatric disorders. Neurological examination was unremarkable except for hemispatial neglect and mild cognitive impairment, characterized by executive dysfunction, reduced verbal fluency, and impaired delayed recall on the Montreal Cognitive Assessment (MoCA), with a score of 24/30. After hospital admission, persecutory ideation persisted, accompanied by false identifications. She became mistrustful, irritable, and agitated. The patient reported elemental (“colourful lines”) and complex visual (zoopsia), as well as auditory hallucinations, particularly running commentary. She described hypnagogic hallucinations in which she heard “skull-crushing noises and screams” coming from the infirmary hallway. The patient had insight towards the unrealistic nature of her visual experiences, but insight was only partial towards the auditory component.
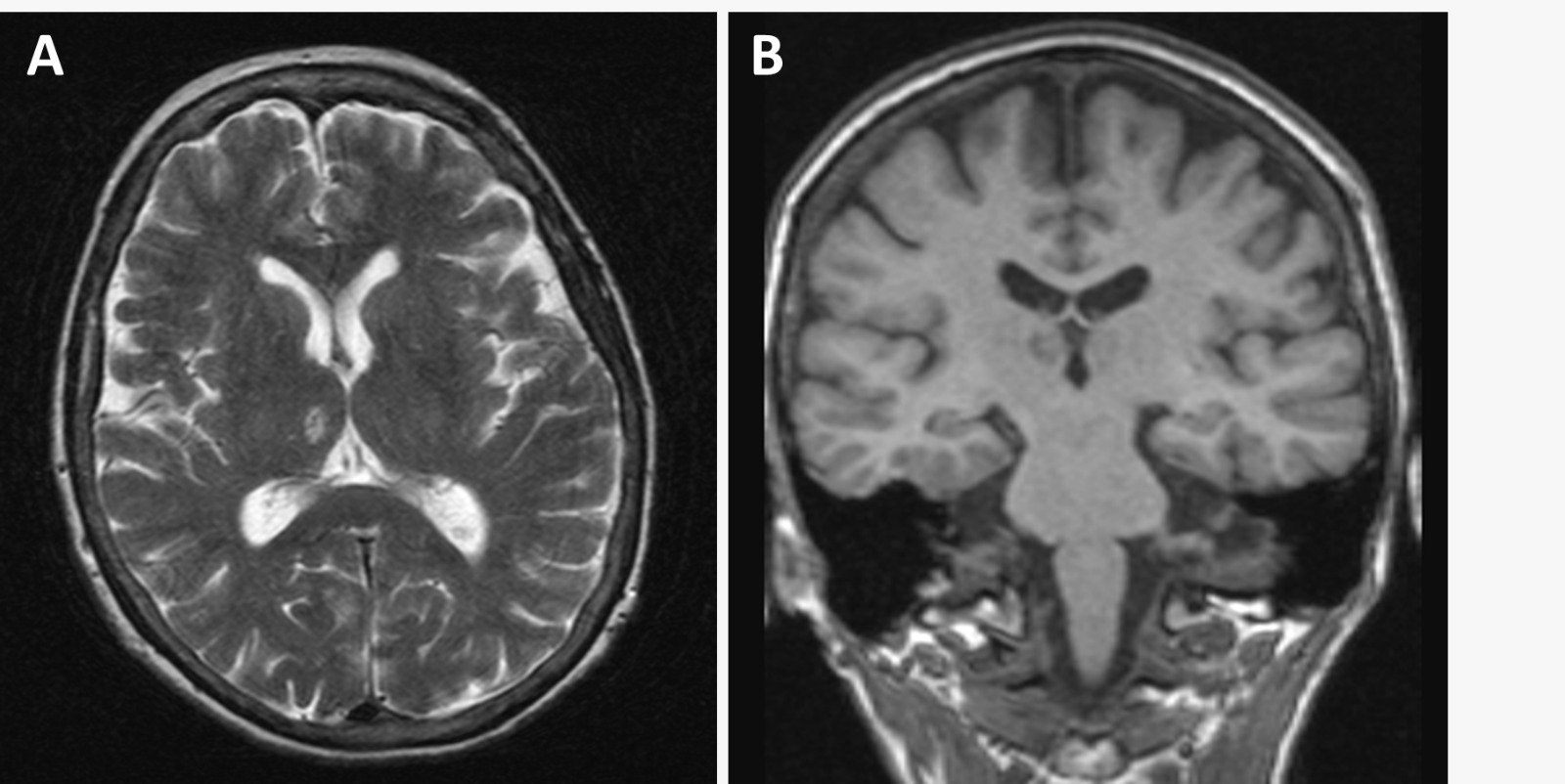
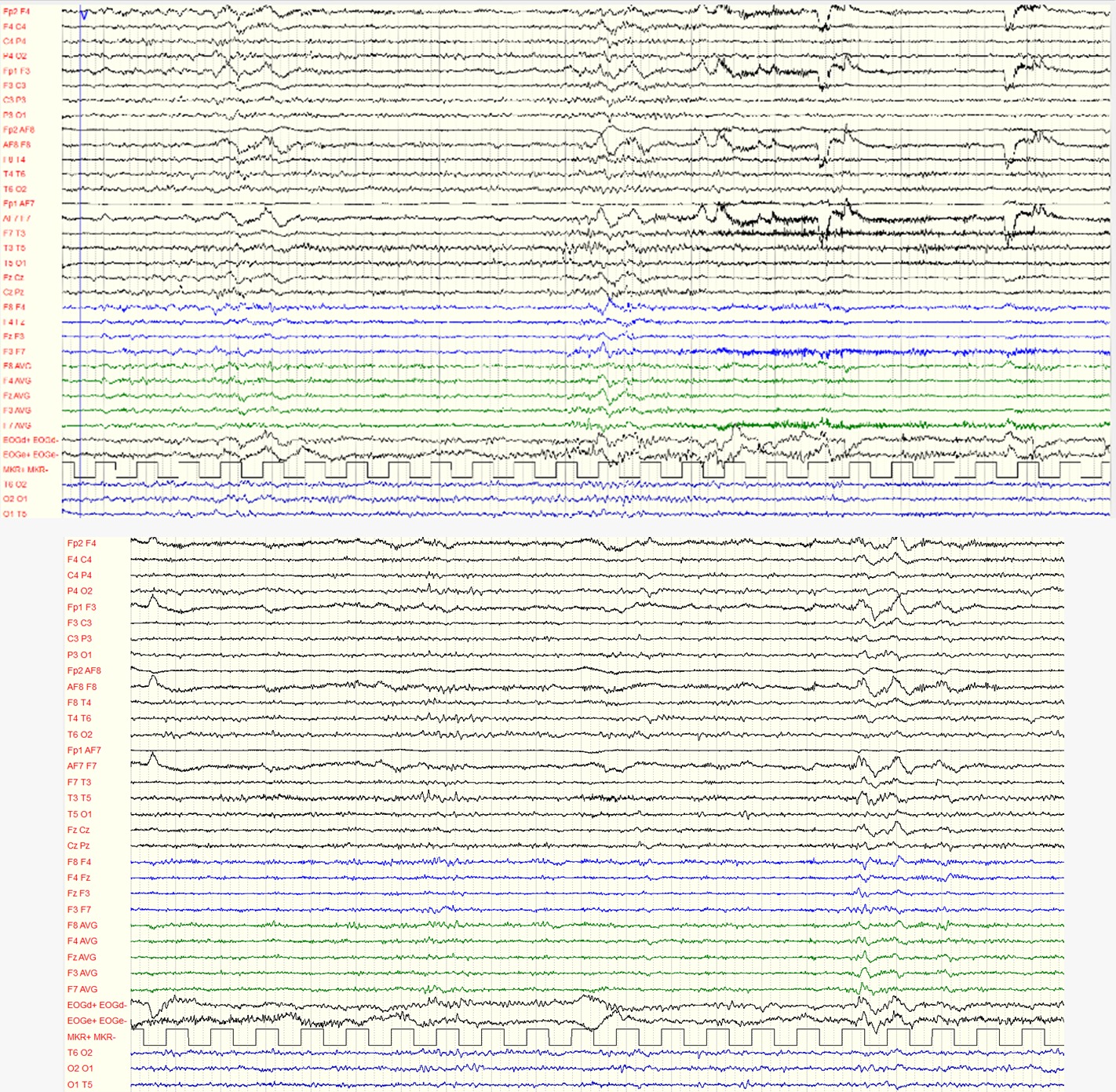
Laboratory workup showed no significant abnormalities, with negative toxicology screening. Brain computerized tomography scan revealed a subacute ischemic lesion in the right c, later confirmed by magnetic resonance imaging (Figure 1A-B). Blood and cerebrospinal fluid (CSF) tests were normal, including polymerase chain reaction and serology for central nervous system infections, neurological autoimmunity and CSF biomarkers (amyloid beta protein, total, and phosphorylated tau). Carotid and vertebral Doppler ultrasonography excluded unstable atherosclerotic plaques and clinically significant vascular stenosis, while a twenty-four-hour Holter monitor study excluded atrial fibrillation. Electroencephalography (Figure 1C) indicated mild diffuse cerebral dysfunction with more significant functional repercussion in the frontal lobes.
_and_t1_(b)_weighted_magnetic_resonance_imaging_scan_(mri)_of_the_brain_performed.jpeg)

The final diagnosis was ischemic stroke due to small vessel disease. Treatment included antiplatelet and statin for secondary stroke prevention. Quetiapine was initially prescribed but proved ineffective. Olanzapine was subsequently initiated and titrated to 15 mg/day, resulting in a marked improvement in psychotic symptoms, with complete resolution within a few days. At the six-month follow-up, the patient remained asymptomatic and had resumed normal daily activities. Two years after the initial onset of symptoms, olanzapine was discontinued, leading to a recurrence of psychotic symptoms, which promptly resolved following the reintroduction of antipsychotic therapy. Given its more favorable metabolic profile, risperidone was selected to replace olanzapine.
DISCUSSION
The infarct affected the medial region of the right thalamus, supplied by the paramedian artery, which serves the dorsomedial nucleus (MDN), internal medullary lamina, and intralaminar nuclei. Paramedian artery stroke can lead to neuropsychological disturbances such as arousal impairment and behavioural changes. MDN lesions have been linked to episodic memory, delayed recall and recognition impairment as well as confabulation.3,4 Left-side infarcts may cause language impairments, while right thalamic lesions can result in visual-spatial deficits, including hemispatial neglect.5,6
The MDN is one of the largest association nuclei of the thalamus, connecting various areas of the prefrontal lobe and the anterior cingulate cortex. It plays a crucial role in cortico-thalamo-cortical loops for integrating multiple cognitive processes and modulating cortical synchrony. Additionally, the thalamus receives inputs from subcortical structures like the amygdala and pallidum, with the reticular thalamus establishing extensive interconnections. These inputs may modulate the information relayed to the prefrontal cortex, suggesting that the MDN also impacts the activity of other thalamic nuclei.7 This might help to understand the impairments shown by our patient in higher-order cognitive processes such as decision-making. Furthermore, the MDN has also been implicated in a fronto-striatal-thalamic network involved in categorization uncertainty,8 which could possibly help explain the autobiographical doubts and general indecisiveness displayed by our patient.
The notable aspect of this case was the emergence of new-onset psychotic symptoms, which are uncommon in lacunar thalamic infarction. Previous case reports have documented sudden hallucinations and delusions arising from unilateral or bilateral lesions in different thalamic nuclei, including the pulvinar, dorsal lateral, dorsomedial, and intralaminar nuclei.9 The visual and auditory hallucinosis are likely due to the release of cortical activity in the extrastriate visual cortex and in the superior temporal gyrus resulting from the loss of thalamic inhibition. These cortical abnormalities appear to be more closely related to the clinical presentations than the original lesion location, once again highlighting the importance of functional connectivity studies.10
In peduncular hallucinosis, insight is typically preserved, as seen in our patient’s visual anomalies. However, insight into auditory hallucinations was only partial, eventually resulting from disruption in the extensive connections of the MDN with the prefrontal cortex, which are important for belief evaluation, especially given the laterality of the lesion and the importance of the right hemisphere in anosognosia.11
Moreover, a previous study12 suggested that the thalamus plays a role in transitioning between internal and external awareness in decreased awareness states. This could also explain the complex hypnagogic hallucinations experienced by our patient.
Studies have shown abnormalities in thalamic structure, connectivity, and neurochemistry in schizophrenia spectrum disorders (SSD), establishing the thalamus as a critical node in the pathways relevant to the development of psychotic symptoms and a candidate biomarker for psychosis.2 A substantial volumetric decrease in several thalamic nuclei, including the MDN, was found in patients with SSD, and a reduction in MDN volume correlated with the severity of positive symptoms.13
As research trends are shifting from brain structure to functional connectivity, so is our understanding of SSD, with the emergence of the triple network model of schizophrenia. This model focuses on dysconnectivity involving the default mode network (DMN), the Executive Control Network (ECN) and the Salience Network (SN), with abnormalities the latter leading to disruption of the normal anticorrelation between the DMN and the ECN. Parts of the MDN are included in the thalamic DMN and SN,14 and several studies have pointed to the MDN as a major driver of the dysconnectivity observed in SSD.15
The thalamus’s role in psychosis can also be analyzed within the thalamocortical dysrhythmia (TCD) framework, which postulates that hyperpolarized thalamocortical neurons exhibit abnormal resting-state oscillations, leading to a shift from the normal α rhythm to a low-frequency (δ or θ) rhythms. This results in the “edge effect”: increased high-frequency activity (γ) in the neighbouring cortex and enhanced theta-gamma coupling (TGC). A recent study found that patients with SSD displayed elevated TGC in the right parietal and frontal lobes and bilateral limbic lobes, with higher TGC correlating with more severe psychotic symptoms.16 Quantitative electroencephalography measures have been proposed as predictors of clinical outcomes in at-risk individuals, as subjects who later developed psychosis exhibited higher theta and delta activity in frontal and central scalp locations and lower alpha peak frequency in occipital-parietal areas.17
The thalamus, along with other subcortical nuclei, is integral to the SN, which mediates switching between the DMN and the frontoparietal or ECN. The triple-network model of psychopathology posits that dysfunction in network switching underlies several psychiatric symptoms, including psychosis. SN dysregulation, in this instance through lesion to the dorsomedial nucleus of the thalamus, may thus impair dynamic switching between the DMN and FPN. The attribution of relevance- or salience- to irrelevant stimuli would thus underlie psychosis.
To date, there are no studies relating TCD to DMN connectivity abnormalities in psychosis. Further research is needed as the DMN has been implied in self-referential processes and daydreaming.18 This could explain the attribution of threatening self-referential meanings to innocuous stimuli, a characteristic of persecutory ideation that may be linked to challenges in transitioning between the DMN and the ECN. Case reports and lesion studies might constitute empirical support for these theories.
Antipsychotic medications may provide symptomatic relief in patients who require pharmacological treatment. Risperidone is more commonly used, but olanzapine and quetiapine have also shown positive results.19 In this particular patient, who had not only struggled with insomnia before admission but also had important hypnagogic hallucinations, sedative effects were paramount both for ensuring sleep quality and improving therapeutic adherence in the presence of partial insight. As a first trial with quetiapine was ineffective, olanzapine combined pleasant antihistaminergic sedation with an incisive profile provided by more potent D2 binding and 5HT2A antagonism, allowing effective control of psychotic symptoms.20 However, as chronic olanzapine treatment is associated with metabolic side effects, its use in a stroke patient requires close monitoring.
Conclusion
This case emphasizes the importance of thalamic information processing in the emergence of psychotic symptoms, supporting recent research findings regarding thalamus’s role in large-scale network dysconnectivity, while also underscoring the need to rule out secondary causes in patients with an atypical presentation of psychotic symptoms.
Ethical Considerations
The patient signed a paper consent form indicating that her case would be discussed in academic journals after removing any identifying information. This case report adhered to the Clinical Research and Ethics Committee’s regulations and the Helsinki Declaration of the World Medical Association.
Disclosures
All authors have no conflicts of interest to disclose.
Funding Source Declaration
All authors have not received any financial support for the research, authorship and/or publication of the article.
Author Contributions
All authors have approved the manuscript and agree with its submission to the International Journal of Psychiatric Trainees.
Acknowledgements
Authors did not declare any acknowledgements.