
INTRODUCTION
The World Health Organization (WHO) declared the novel coronavirus infectious disease (COVID-19) a pandemic on 11th March 2020. Severe lockdown measures were rapidly adopted in spring 2020 in almost every European country.
Mental health, particularly among young adults, was severely affected during the lockdown in the spring of 2020. Short-term consequences of the pandemic in young adults have already been shown in the literature, such as the increase in reported psychological distress,1,2 higher rates of depressive and anxiety symptoms,3 and the increase in mental health care needs related to lower resilience.4 Social isolation due to restrictive measures represented a stressor. Li et al.5 provided quantitative evidence that, during the COVID-19 pandemic, social support was more significant to the resilience and mental health of emerging adults than older adults.
As social isolation increased, psychological distress was more likely to occur in young adults.6 Loneliness and social isolation are prominent risk factors for both anxiety and depression.7,8 In a large European longitudinal study conducted between March and July 2020 in four countries, higher levels of loneliness were found in young adults compared to other subgroups of the population.9 Social isolation measures are strongly connected with loneliness, and these two elements were proven to increase the risk of depression and possibly anxiety in the short and long term.10 Thus, loneliness and social isolation are dynamic experiences and time-variant, influenced by different social relationship trajectories, including prolonged exposure to isolation or changes in loneliness.11
Protective factors, such as resilience, play a crucial role in mental health outcomes.12 Resilience, the individual’s ability to healthily cope with adverse life events, impacts anxiety and depression.13 It has previously been described as an essential target to reduce the damage-function from stressful events.14 A recent mediation model explained how resilience prevents stress from developing into depressive symptoms, and this could be direct, or mediated by anxiety symptoms.15
Concerning the interaction between resilience and loneliness, Jakobsen et al.16 showed that loneliness was significantly and negatively correlated with resilience, indicating that young adults who present higher levels of resilience tend to feel less lonely. In addition, resilience was predicted by both loneliness and life satisfaction in a sample of university students.17 To date, we are not aware of any published studies assessing the relationship between these two factors during the COVID-19 pandemic.
Since the social isolation measures intended to flatten the COVID-19 curve can be considered a stressor, assessment of the medium and long-term effects on young adults’ mental health is needed.3 In particular, the role of risk and protective factors, such as loneliness and resilience, respectively, should be explored during this pandemic context to better understand their impact on mental health.
Previously, we studied 825 emerging adults aged between 18 and 25 years in both Belgium and Italy during spring 2020. At that time, lockdown revealed a 5% increase in mental health care needs in this population, associated with lower resilience.4
Study objectives
We proposed a prospective longitudinal study to evaluate the effects of a COVID-19 pandemic-related stressor on young adults’ mental health, social isolation. In particular, we aimed to assess the potential positive impact of the slackening of social isolation measures. Firstly, we aimed to evaluate whether loneliness decreased according to mental health care needs status between the COVID-19 lockdown measures phase in spring 2020 (T1) and during summer 2020 (T2), when these measures were softened in most European countries. The second goal of this study was to test the potential positive linear correlation of the difference in loneliness scores with resilience competencies in this population of emerging adults.
MATERIALS AND METHODS
Ethics and dissemination
This study was approved by the Institutional Review Board (IRB) of Erasme Hospital, Belgium (EC identifier P2020/245) and the IRB of the Department of Brain and Behavioral Sciences of the University of Pavia, Italy.
The study was conducted in accordance with the International Conference on Harmonization (ICH) for Good Clinical Practice (GCP), and it was registered on ClinicalTrials.gov (Identifier: NCT04371250).
All participants gave their written consent to participate in the anonymous two-phase survey.
Procedures and recruitment
The online survey was managed on the secure REDCap© (Research Electronic Data Capture) platform. Data collection was carried out twice. The first assessment (T1) was conducted from 7th April to 4th May 2020, while restrictive measures, such as social isolation, were active in Italy and Belgium.4 Even if the restrictive measures might not have been identical in Italy and Belgium, forced social isolation measures in the first COVID-19 wave were very similar in all Western European countries. At T1, the recruitment was based on snowball sampling: via e-mails, homepages of community groups, and social media platforms such as Facebook, WhatsApp and Instagram. Each recruitment message included a brief explanation of the general study aim (i.e., investigating the impact of forced social isolation on young adults’ mental health status) and a link to the online survey. At T1, once they clicked on the link, participants were initially presented with the information sheet and the consent form. At the end of the T1 online survey, participants were asked to give their consent and to provide their email addresses to participate in the T2 follow-up survey.
Consenting participants were invited by a personal e-mail to participate in the second assessment (T2). T2 took place between 3rd August and 10th October 2020, three to five months after the end of lockdown measures, including forced social isolation (in Belgium, 18th May, and Italy, 23rd May). At T2, once participants clicked on the link, the informed consent form appeared before the survey questions. Full-time completion was estimated at 15 minutes.
Participants included in the study were both male and female, aged from 18 to 25 years, French or Italian speaking, resident in Belgium or Italy, and those who gave informed consent. Surveys that were incomplete or filled after the lock-down measures in the country of residence ended were not considered for analysis.
Materials
At both T1 and T2, the online survey comprised four sections. The first section was conceived to collect socio-demographic data (gender, age, relationship status, country, housing and occupation). The second section consisted of the daily habits during forced social isolation measures (at T1) and after the end of these (at T2), such as a change in daily occupation, housing, and online (i.e., phone calls and social media) and offline contacts (i.e., face-to-face) with family and friends. The third section assessed the mental health care needs before, during, and after the lockdown measures, such as receiving psychiatric care (outpatient and/or inpatient), care from other mental health professionals, and use of prescribed psychotropic drugs. The fourth and last part explored loneliness (T1 and T2) and resilience (T1) through two self-reported scales.
University of California Los Angeles (UCLA) Loneliness Scale
The UCLA Loneliness Scale consists of a 20-item self-report scale.18 Participants are asked to report how frequently (from 1=never to 4=always) they experience distinct loneliness feelings in their lives. Some items are scored inversely and shuffled within the questionnaire. Higher overall scores represent greater loneliness.
Validation of this questionnaire has been carried out for both Italian-speaking and French-speaking populations.19,20 As previous studies revealed that levels of loneliness can vary in relation to different life circumstances,21,22 loneliness scores were re-evaluated at T2. Change in loneliness has already been described in the scientific literature, especially in older people, to assess its relationship with physical health deterioration23 or with the protective role of arts activities.24
Resilience Scale for Adults (RSA)
The RSA is a 33-item self-report measure.25,26 The revised version of the RSA, a 7-point semantic differential scale,27 was used for this study. Inversely scored items are shuffled in the questionnaire. The measure is composed of six intrapersonal and interpersonal factors of resilience.27,28 The first four factors, (1) Perception of self, (2) Planned future, (3) Social competence, and (4) Structured style, explore the personal abilities of each participant. (5) Family cohesion measures family support and (6) Social resources assesses the availability of social support.29
The total RSA score is a global index of resilience. Higher scores indicate higher levels of resilience. This scale is validated in both Italian-speaking30 and Belgian French-speaking populations.29
In our study, we decided to analyze both RSA total and factor scores to better understand the protective role of global resilience and to examine which component influenced the variation in loneliness.
Groups
Participants were divided into three groups according to information about their mental health status. Individuals who had never sought mental health help were assigned to Group 0. Group 1 consisted of young adults who had previously experienced mental health care, but did not face any change in this care during the pandemic period. Group 2 represented young adults who had experienced an increase in mental health care needs from the beginning of social isolation measures, such as their first ever contact with a mental health professional, the beginning or augmentation of psychotropic medication, or inpatient psychiatric care.
Statistical Analysis
All statistical analyses were conducted using the software Stata/MP 14.1.
Descriptive statistics were performed to study sociodemographic characteristics of the sample at T2 and within each group: absolute and relative frequencies were presented in the categories of qualitative variables; means with standard deviations were used to describe normally distributed quantitative variables. The normality of distributions was assessed with graphical representations (histogram, box plot, and normal plot).
The frequencies in categories were compared between groups with Fisher’s exact test. The homogeneity of variances between groups was verified with Levene’s test, and the means were compared with an analysis of variance (ANOVA).
We analyzed the outcome difference in the UCLA scale total score between T1 and T2 according to potential explanatory variables with linear regression. We presented regression coefficients (b) and 95% confidence intervals. We then performed multivariable analyses and tested all combinations of explanatory variables to choose the best model based on the Akaike information criterion (AIC). The best model included just the group and the resilience score. This corresponded to an analysis of covariance (ANCOVA).
Along with linearity, we verified normality and homogeneity of variances of residuals with graphical representations, homogeneity of slopes in groups by testing interaction in the model, and independence between factor and covariable with Kruskal-Wallis test. The p-values of post-hoc pairwise comparison tests were adjusted with Bonferroni’s method. The statistical significance level was set at 0.05.
RESULTS
Participants
At T1, 1285 people filled out the online survey. According to the inclusion criteria, 460 responders were excluded, and the final sample at the T1 consisted of 825 participants. Results from T1 were described in a previous paper.4
Among these participants, 251 gave their consent to be contacted at T2. At T2, 95 participants accessed the online survey. However, 7 of the previous participants did not provide their consent or did not fill out the survey. Therefore, the final sample at T2, on which the analyses were conducted, consisted of 88 participants (retention rate of 35%).
Demographic and clinical data
The majority of participants in this longitudinal study were female (78.4%), but sex difference was not statistically significant among groups (p-value=0.29).
Following the inclusion criteria, the age range was between 18 and 26 years old, mean (SD) = 22.0 (2.4) years, and consisted of 47 (53.4%) participants living in Italy during and after the lockdown measures and 41 (46.6%) living in Belgium. Within the sample, 41 (46.6%) participants were single and 47 (53.4%) in a relationship.
The participants’ main occupation during their daily lives was distributed as follows: 72 (81.8%) participants were students; 11 (12.5%) were working and 5 (1.3%) did not have any occupation or reported other activities than study or work. Concerning the distribution among the three groups, group 2 (increased mental health care needs) was composed of six respondents, group 0 (no mental health care needs) represented less than half of the assessed young adults (n=33) and group 1 (constant mental health care needs) was the most represented (n=49). No significant difference in sociodemographic characteristics was found between groups, but we might have lacked power to find significant differences in group 2 due to the small size of that group.
Analyses of difference in loneliness
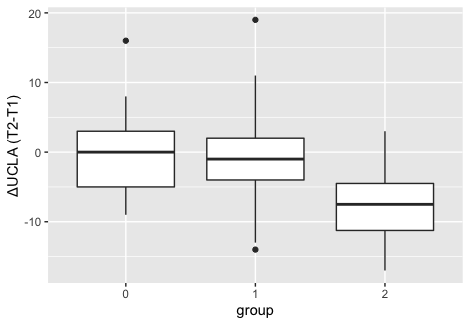
The difference in the UCLA scale total score according to groups and contextual data is shown in Table 1. The decrease in loneliness score from T1 to T2 was statistically more significant in participants belonging to group 2 compared to both groups 0 and 1 (adjusted p-value=0.02 and 0.01 respectively). The distributions of difference in loneliness scores are graphically represented in Figure 1.
In participants presenting higher baseline scores in the RSA total (p-value=0.03) or in the RSA structured style factor (p-value=0.02), the UCLA scale total score decreased less between T1 and T2.

Analysis of covariance of loneliness according to group and resilience
Covariance analysis of the difference in loneliness score between T1 and T2 according to the mental health care group and resilience is reported in Table 2.
These results show that the difference in the UCLA scale total score was significantly associated with the mental health care group (p-value = 0.02) and with the RSA total score (p-value=0.02). Again, loneliness score significantly decreased more from T1 to T2 in participants belonging to group 2 compared to both group 0 (adjusted p-value=0.02) and 1 (adjusted p-value=0.01). These results are graphically represented in Figure 2. The slope for variation of the loneliness according to resilience appears to be different between groups, with group 2 having a steeper slope, but the interaction between groups and resilience score was not significant (p=0.16), probably because of the small sample size in group 2. Thus, we chose to keep a model without interaction.

DISCUSSION
This study aimed to evaluate the medium-term variation of loneliness in young adults in line with the slackening in forced social isolation measures in Italy and Belgium during the COVID-19 pandemic. In this section, we will discuss findings about the impacts of social isolation on loneliness, the protective role of resilience, contextual factors, and future perspectives. The prospective longitudinal design and the sampling in two different European countries are significant strengths of this study.
The impacts of social isolation on loneliness
Loneliness was greater in young adults with active mental health care needs during COVID-19 lockdown measures in spring 2020, supporting the hypothesis that social isolation represents a strong negative stressor in case of pre-existing psychological discomfort.4 There was a general decrease in UCLA loneliness scale total scores from T1 to T2 in young adults with mental health care needs (both groups 1 and 2). Social isolation measures are strongly connected with loneliness, and they both increase the risk of depression and anxiety in the short and long term.10 Our results show that the slackening of social isolation measures was associated with a decrease in feelings of loneliness in this population.
In detail, the decrease of UCLA scale total scores from T1 to T2 was statistically significantly different in group 2 (increased mental health care needs) compared to both group 0 (no mental health care needs) and 1 (constant mental health care needs). Thus, young adults who experienced an increase in mental health care needs during lockdown measures in spring 2020, showed a greater reduction in loneliness during summer 2020, when social restriction was slackened. Loneliness in participants from group 2 appears to depend more on their liberty to manage social interactions compared to young adults who did not experience an increase in mental health care needs. Loneliness has already been connected to various psychiatric conditions and psychosocial risk factors.31 Specifically, the duration of loneliness, more than its intensity, has been strongly correlated with mental health symptoms, such as anxiety and depression.10 These results support the evidence that interpersonal social interactions might particularly benefit vulnerable young adults by reducing loneliness. In addition, participants with increased mental health care needs should have received care. This intervention could also play a positive role in the loneliness reduction in the evaluated period.
The protective role of resilience
Resilience represents a protective factor from the effect of stress leading to symptoms of depression during the COVID-19 pandemic, either directly or mediated by anxiety.15
It is already evident in the literature that resilience and loneliness are negatively correlated.16,32,33 Loneliness, together with life satisfaction, predicts resilience.17 To the best of our knowledge, the present study is the first to evaluate the interaction of resilience and loneliness in young adults during the COVID-19 pandemic.
Total scores of RSA (T1) were positively correlated with the difference in UCLA scale total scores from T1 to T2 in the evaluated population. High resilience competencies were significantly connected to a lesser variation in loneliness in our sample after slackening of social isolation. On the contrary, a greater decrease in loneliness was found to correlate directly with lower RSA total scores. These results highlight the negative correlation between resilience and loneliness. Participants with lower resilience at T1 experienced a greater positive effect on loneliness when the stressor of social isolation was removed. Even if the interaction was not statistically significant, the variation of UCLA score according to RSA total score was not similarly sloped in the three groups (Figure 2). The association between resilience and change in loneliness appears to be more critical within young adults with higher mental health care needs (group 2). This element suggests that the reduction of loneliness seems greater when connected to lower resilience abilities in participants who experienced an increase in mental health care needs.
In addition to results regarding RSA total scores, the RSA Factor 4 (Structured style), which measures the preference to have clear goals and routines,29 was the only factor that linearly correlated to a more remarkable change in UCLA scale total scores from T1 to T2. This resilience factor could play a specific role in the context of the COVID-19 pandemic in the sense of adaptive abilities.4 Daily routines and plans were considerably disrupted due to social isolation. Since the COVID-19 outbreak, the scientific community has focused on the role of daily living, aiming to promote psychological resilience.34 Some individuals, whose resilience competencies were mainly connected to their abilities to have and follow routines, might have struggled to adapt their daily living in the context of forced social isolation. Interestingly and coherently to this crucial point, during the slackening of social isolation span (T2), the RSA Factor 4 appears to be the only resiliency sub-factor statistically correlated with a more consistent variation in loneliness in our sample.
Contextual factors
Social contacts are known to reinforce coping with difficulties, fears, and worries. The liberty to have interpersonal interactions and to spend social moments with others revealed a greater positive impact on participants with lower resilience competencies.35 These findings suggest that these responders displayed less ability to cope with social isolation in spring 2020. In this period of increasingly virtual exchanges, it is essential to stress the protective role of interpersonal social support on both physical and mental health.36 Mental health, especially in young adults, is connected to peer group interactions.37 Even if online social contacts were possible during forced social isolation, offline peer-to-peer contacts revealed to be a protective factor against the increase in mental health care needs.4 No other contextual factor, such as being in a couple, occupation, or country, was found to be influential in the variation of loneliness.
Medium-term effects and future perspectives
The forced social isolation to flatten the COVID-19 pandemic curve can be considered a stressor.38 It is important to focus on the medium to long-term psychological impacts of this burden beyond any immediate discomfort. Lower resilience competencies combined with a continuous medium-high intensity stressor could result in long-term symptoms. Since we are facing an unprecedented situation in modern society, future research should focus on medium to long-term clinical mental health implications of the COVID-19 pandemic and associated restrictive measures.
In this longitudinal study, resilience was a predictor of positive medium-term outcomes in terms of loneliness. Therefore, resilience competencies represent a fundamental protective factor for mental health to reduce the impact of negative feelings, such as loneliness, on psychological well-being.16,17 Some authors have already developed a model to predict psychological resilience during the COVID-19 lockdown.14 Their findings seem to support an intervention in non-cognitive skill development to prevent the damage-function from adverse events. This evidence might influence decision-making organizations and mental healthcare managers to invest more in the preventive approach. Practical actions are needed to reinforce resilience competencies and to allow the protective function of interpersonal social support to act positively on psychological discomfort.
It might be appropriate, for clinical reasons, to promote the rapid assessment of resilience competencies in future large-scale disasters. Identifying individuals who display lower resilience competencies could result in the early detection of potentially at-risk people, permitting targeted interventions and psychological support.6 A proactive attitude in mental health care institutions might contribute to reducing stigmatization and ease the help-seeking process.
Limitations
Certain limitations in this study should be recognized. The UCLA loneliness scale has been validated in French-speaking Canadians, and this might underestimate the cultural dimension of loneliness among the Belgian sample. Additionally, even if the longitudinal design of the study represents a strong construct, the respondents’ drop-out was considerably high. This phenomenon constitutes two main biases. On one side, the final sample was small, particularly regarding participants from Group 2. Additionally, there was probably selection bias; in fact, participants needed to be motivated to answer questions about their mental health status and psychological vulnerabilities. It is possible that some responders dropped out of the study for two opposite reasons, either their psychological discomfort was too high, or they did not feel mental health was a priority during the considered period. This research was explorative and its results need to be confirmed in future studies with larger groups.
CONCLUSION AND IMPLICATIONS
This study presents an assessment of the medium-term variation of loneliness in emerging adults (18 - 25 years old) in the COVID-19 pandemic context from the period of active lockdown measures in spring 2020 until the slackening of forced social isolation during summer 2020 in Italy and Belgium.
The two subsequent changes in the liberty to manage personal social contacts have been remarkable events in the history of the world. The longitudinal evaluation of variation in loneliness according to this constraint, external and commonly shared among all participants, resulted in an interesting model to relate loneliness to social interactions.
A decrease in loneliness during the summer of 2020 was generally reported in all participants with mental health care needs. Remarkably, the exploratory analysis showed that the most significant decrease happened in individuals who experienced increased mental health care needs during the lockdown measure in the spring of 2020 and, thus, forced social isolation. This result shows the positive role of the right to interact socially with others on young adults experiencing psychological discomfort while most in-person relationships were not allowed. In addition, resilience and longitudinal variation in loneliness are directly correlated. Lower resilience competencies could be considered as predictive of a medium-term change in loneliness in the context of external constraints limiting social interactions.
This prospective longitudinal study, carried out through a double-phase online survey, demonstrated the importance of rapid assessment of mental health during large-scale disasters of both immediate and medium-term outcomes. Early detection of psychological distress may be an accurate way to offer targeted interventions to at-risk emerging adults and guarantee a medium-term positive impact on mental health. Since the COVID-19 pandemic continued and additional social restrictive measures were established after the summer of 2020, further research should focus on medium to longer-term effects on young adults’ mental health care needs.
ETHICS APPROVAL
This study was approved by the Institutional Review Board (IRB) of Erasme Hospital, Belgium (EC identifier P2020/245) and the IRB of the Department of Brain and Behavioral Sciences of the University of Pavia, Italy.
DECLARATION OF CONFLICT OF INTEREST
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
ACKNOWLEDGMENTS
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The study was carried out as part of the University Chair “Psychiatry in Transition in a World in Transition” (Université Libre de Bruxelles - ULB) with the support of Julie Renson Fund, the Queen Fabiola Fund and the King Baudouin Foundation [grant number 2019-J1130650-213107].