Portugal faces diverse challenges in terms of mental health care due to several inter-related factors affecting the mental well-being of the population. Estimates of the prevalence of lifetime mental disorders in Portugal are alarmingly high, exceeding 30%, accounting for 11.7% of disease-adjusted life years (DALYs) lost, according to the national survey on mental health.1 Compared to other European countries, the estimated prevalences are higher: 7.9% for depression, 16.5% for anxiety, 3.5% for impulse disorders, and 1.6% for substance abuse.2 Regarding the latter mental condition, alcohol consumption is widely accepted but it is known that approximately 20% of male suicides in Portugal can be attributed to its misuse.3
Besides the highly prevalent conditions, there are some geographical factors contributing to health and social inequalities. Rural regions, for instance, present scarce resources and limited opportunities, grappling with economic hardships, which contribute to feelings of loneliness, hopelessness, low self-esteem, disengagement from the community, and distress among the population, namely heightened stress, anxiety, and depression.4 In these regions, the lack of health resources also impairs access to mental health care when needed. The stigma surrounding psychiatric care remains a considerable barrier to mental health support in Portugal, probably because of a low level of mental health literacy.5 This pervasive stigma further complicates the landscape of mental health care in Portugal, hindering individuals from accessing timely and appropriate support.6
As psychiatric trainees, we feel a need to deal with all these social and geographical aspects that are intrinsically related to our patients’ mental health, forcing us to reflect on the national mental health policies. In response to the pandemic’s impact on European economies, the European Council introduced the Next Generation EU, forming the basis for the Recovery and Resilience Mechanism (RRM).7 Portugal’s plan, an integral part of RRM, focuses on strengthening the National Health Service, emphasising improving mental health care quality, particularly for vulnerable populations.7 At the heart of this transformation lies the inception of Community Mental Health Teams (CMHTs), an inventive care paradigm aligned with the principles of the National Mental Health Plan (PNSM).7 The PNSM focuses on:
-
Ensuring equitable access to high-quality mental health care for all individuals in the country.
-
Upholding human rights, dignity, and respectful care for those with mental health issues.
-
Reducing the impact of mental disorders on individuals and society while promoting mental well-being.
-
Decentralizing mental health services to bring care closer to communities and involve patients and families.
-
Integrating mental health care into the broader healthcare system to improve access and reduce institutionalisation.
Thus, Community Mental Health Teams (CMHTs) provide a multifaceted approach to care, addressing interconnected issues, and the PNSM highlights the commitment to addressing the clinical aspects and the broader social and human rights dimensions of mental health care.6
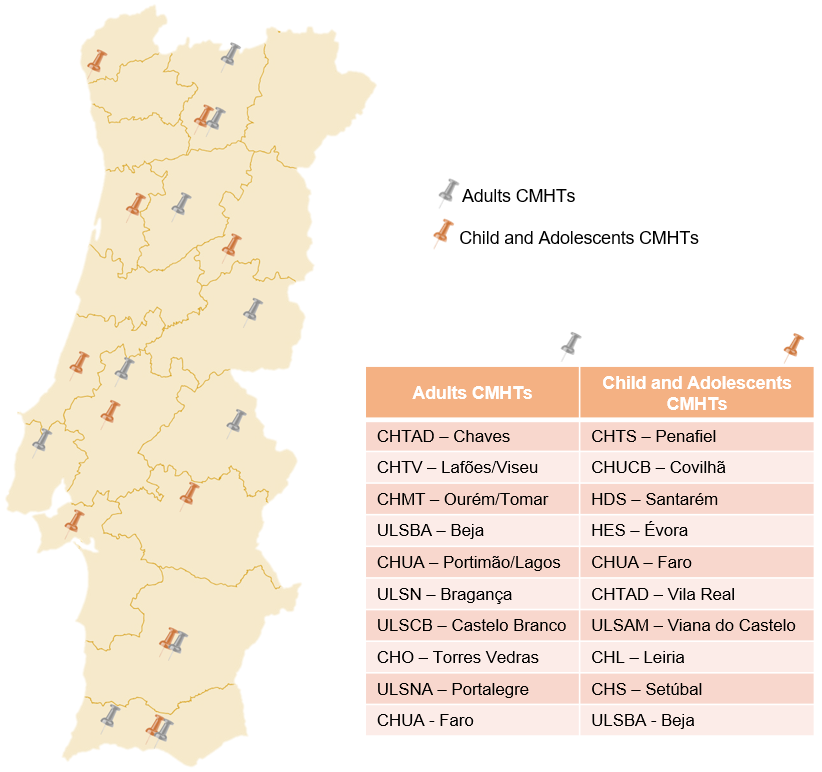
The CMHTs, as shown in Figure 1, are distributed in all five regional health administrations, catering to adult and child/adolescent populations. Notably, CMHTs prioritise isolated regions within the country’s interior, rather than major urban centres.
.png)
Comprising a diverse range of specialists, including psychiatrists, specialised nurses, psychologists, social workers, therapists, and technicians, these multidisciplinary teams are tailored to address the unique needs of their patient groups.7 Their mission involves coordinating care within local communities, primarily for individuals with severe mental health conditions. It is expected that CMHTs will expand their outreach to serve specific patient groups in the future.7
The establishment of CMHTs is still recent and there is still no published evaluation of their activity regarding short and long-term results. To conclude, CMHTs, with their interdisciplinary approach and integrated care, offer a strategic response to these multifaceted challenges. However, there is a concern about insufficient human resources to realise the full potential of CMHTs. As trainees, the fact that the psychiatry residency program includes three months of community psychiatry reflects the intensified emphasis on community-rooted care. We also believe that experiencing this reform during the training process is an advantage, as we are currently in contact with a new organisation of mental health services. However, we believe it would also be important to assess patients’ and caregivers’ perspectives about the work of CMHTs because the reforms aim to improve people’s healthcare.
Declaration of Interest
The authors have no interests to declare.
Role of funding sources
The authors have no funding sources to declare.
Author contributions
VHS was responsible for the design of the study, literature review, writing the manuscript and revision of the manuscript. MP was responsible for image design, literature review, manuscript writing and manuscript revision. BJ, IAS, and FSM were responsible for the literature review, writing the manuscript and revision of the manuscript.
Ethical approval was not required for this work.