1. INTRODUCTION
Approximately 700,000 people worldwide commit suicide every year, and several more people attempt it.1 Suicide affects every age group, but among individuals aged 15-29 it represents the fourth leading cause of death, and it is pervasive worldwide.1 Suicide is not limited to high-income countries, since more than 77% of suicides worldwide occurred in low- and middle-income countries in 2019.1 Suicide and suicidal behaviours have been found in association with several conditions; however, a considerable number of suicides occur impulsively during periods of crisis when coping with life stresses becomes challenging (such as financial problems, relationship breakdowns, or dealing with chronic pain and illness).1 Moreover, involvement in conflict, experience of disasters, violence, abuse, or significant loss, alongside with a sense of isolation, are strongly correlated with suicidal behavior.1
The relevance of suicide does not remain confined to those who take their own life, but also impacts families and communities. Long-lasting effects of suicide have been widely reported on mental health professionals who experience significant levels of emotional distress after patient suicide (PS).2 These subjects have commonly been referred to as “second victims” or “suicide survivors”.3–5 Mental health professionals may face PS throughout their career: according to the available literature, over a third of psychologists and two-thirds of psychiatrists report this experience.6,7 PS represents a frequent and stressful occurrence, and it can be considered an “occupational hazard” for mental health professionals.3,8 After PS, negative emotional reactions influencing both professional and personal life, as well as symptoms of acute or post-traumatic stress, have been observed among these workers.9,10 On the other hand, it has also been suggested that PS drives psychiatrists to be more vigilant in monitoring higher-risk patients, for instance exploring suicidal ideation more directly and explicitly than before.11
The impact of PS is putatively more traumatic for those in the earliest stages of their careers in mental health care, such as psychiatric trainees and early career psychiatrists (ECPs). Indeed, they may be even more prone to perceive feelings including guilt, shock, anger, shame, and loss of confidence and to encounter troubles in receiving support in the aftermath of PS.8,12–16
Despite the substantial influence of PS experience on mental health workers, there is a glaring absence of dedicated sessions within most psychiatry training programs. Indeed, approximately only 20% to 25% of psychiatry trainees reported having received such training.17–19 Although the need of implementing and strengthening programs addressed to psychiatric trainees and ECPs living the stressful aftermath of PS has been highlighted over time,20,21 evidence on this issue is still scant, and further investigations focused on trainees and ECPs are much needed. Therefore, we conducted a qualitative study aimed at exploring the impact of PS on psychiatry trainees and ECPs in Italy as well as their needs.
2. MATERIALS AND METHODS
2.1. Study design and recruitment strategies
An online survey was developed as a tool for qualitative research.22 It was disseminated through the platform EUSurvey in June 2023. Participation was anonymous and voluntary, without monetary or other incentives. Participants were psychiatric trainees and ECPs working at the Clinical Psychiatry Unit of Polytechnic University of Marche (Ancona, Italy), who had experienced a PS in the previous two months. Eligible participants were requested to complete all sections of the survey. In order to guarantee full anonymity in such a restricted setting, data about participants’ age, gender, and year of training were not collected. An ad hoc Excel spreadsheet was used in order to archive responses. All participants provided informed consent to take part in the study.
Declaration of Helsinki’s ethical principles for Medical Research involving human subjects were followed.23 According to Italian regulations, formal approval from the Ethics Committee was not required for this study since data collection exclusively targeted psychiatric trainees and ECPs, not involving vulnerable populations, and the study employed a non-invasive, observational method (online questionnaire).24
2.2. Measurements
Survey questions were piloted by the Authors (GL, DC, MDV) before starting the study, so as to ensure their understandability and face validity in relation to topics covered. The survey consisted of the following five questions: 1) How did you feel at the news that one of your patients committed suicide?; 2) How do you think this event has influenced or will influence your future work?; 3) Have you felt the need for more support and/or specific spaces and programs to manage event-related experiences? If yes, how could they be organised?; 4) Were your colleagues supportive? What did they do for you upon hearing the news?; 5) Has anyone ever taught you what to do or how to cope with these events? The questions were open-ended and allowed respondents to report personal meanings on a focused topic by using a non-preset format25 without any word limit for the answers.
2.3. Data analysis
A thematic analysis approach, useful in identifying, analysing, and reporting patterns (themes) within data in qualitative research, was used.26 More specifically, the thematic analysis followed these steps: 1) familiarising with the data; 2) generating initial codes; 3) constructing themes and sub-themes; 4) reviewing potential themes; 5) defining and naming themes; 6) reporting of findings.
Since participants provided their answers in Italian, the replies were first analysed and clustered as such. Data were analysed first by each author independently, then through a panel discussion involving all authors to build a consensus on emerging patterns. The data were analysed using a semantic approach, which allows identifying themes at face value, within the explicit or surface meanings of the data, with the analyst not looking for anything beyond what a participant has said or what has been written. This approach allows minimising the influence of investigators’ background and assumptions.26 Finally, the most relevant statements were translated in English by the authors (GL, DC, MDV) for the purpose of reporting and citing in the manuscript.
3. RESULTS
Fifteen subjects (psychiatric trainees and ECPs) completed the online survey.
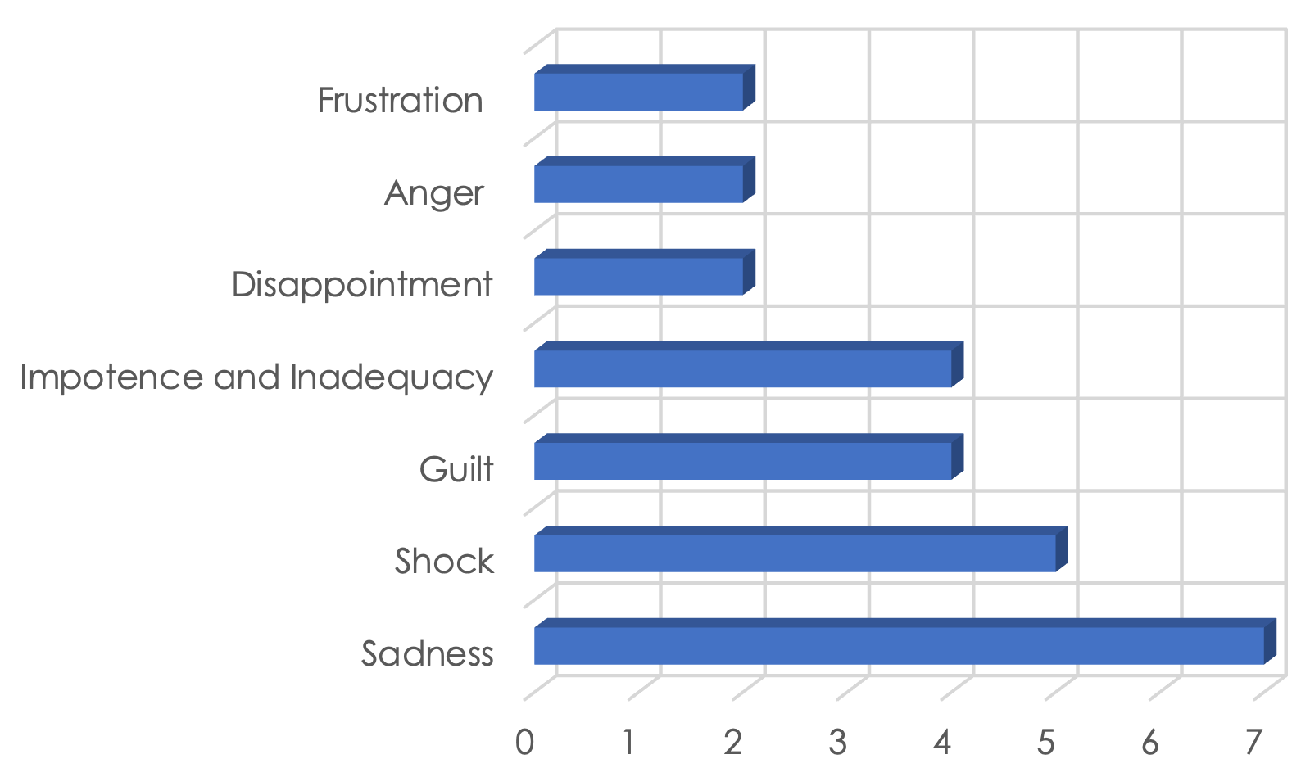
The following three themes were identified: 1) emotional impact of PS; 2) influence of PS on future work; 3) perceived support and management in the aftermath of PS. Themes were further distributed across different sub-themes. Figure 1 displays the feelings more frequently experienced by participants.

3.1. Emotional impact of PS
3.1.1. Sadness. Among all feelings that emerged when respondents were asked how they had felt at the news of the PS, sadness (46.7%, n=7) was the most reported. Sadness was never reported as the sole emotion but as a common thread across individuals also experiencing other feelings ranging from inadequacy to anger. In this kind of situation, the boundaries between professional life and the more private sphere may become less clear.27
“As much as we can give and do our best, some things are larger than us, and it is always sad to lose someone”
3.1.2. Shock. Besides sadness, shock (33%, n=5) – often associated with disbelief and denial (20%, n=3) – was the most reported emotion after hearing of PS. Whether patients were at high risk of committing suicide or, on the contrary, had no warnings or predictors whatsoever, the event may still prove surprising and upsetting for the professional, especially if in the early stages of their career.
“I did not believe it really happened, I felt bewildered, I felt strongly shocked”
3.1.3. Guilt, impotence and inadequacy, disappointment, frustration, and anger. Guilt (27%, n=4) in one of the common emotions experienced by professionals who were close to the patient who committed suicide, especially if shortly before the event. Feelings of impotence and inadequacy (27%, n=4) often accompany guilt. Psychiatric trainees and ECPs may feel that they had “seen it coming” and somehow prevented it but that they had been actually powerless to prevent it in the end.
“Guilt. I felt like I did not do enough”
Together with helplessness and inadequacy, a range of feelings can emerge, from disappointment, to frustration, to anger. These emotions are an integral part of the coping process, and it is not uncommon to struggle with conflicting feelings in the aftermath of such an event.28,29
3.2. Influence of PS on future work
3.2.1. Greater attention. Most respondents stated that PS could be a reason for applying further attention to the patients’ needs and seemingly insignificant details (33%, n=5). Some also reflected on the need for a more in-depth dialogue with the patients (13%, n=2) and for shaking off prejudices.
“I will try to be more attentive and understanding with my patients. I will try to spend more time with them and avoid hasty judgments”
“This has pushed me not to take anything for granted. I aim at giving the same attention and quality of care to everyone, especially to patients with the greatest needs”
3.2.2. Influence on patients. Greater awareness about the psychiatrist’s influence on patients (13%, n=2), but also the feeling of extreme limitation with regard to what can be done for the patient, were reported.
“This event made me question the influence psychiatric trainees and early career psychiatrists have on others”
In particular, one participant declared that he/she was afraid of not being able to make a mark in people’s lives and was therefore considering leaving the job. This was related to feelings of impotence and inadequacy.
“This made me very doubtful about continuing doing this job. I do not think I can leave a positive mark in people’s lives”
3.3.3. No impact. One (7%) respondent declared that PS would not have influenced future clinical work, since such an event remains unpredictable. However, some fear emerged.
“This experience has taught me that suicide is one of the most difficult events to predict so it will have little influence on my current or future work. I will, however, avoid having patients alone in the room”
3.3. Perceived support and management in the aftermath of PS
3.3.1. Emotion sharing and perceived support. Sharing of such emotional experience among peers was reported by most of surveyed subjects (60%, n=9), two stated it was not enough, two declared this topic was still related to fear and reticence, while one reported to have supported others.
“There was a brief, improvised moment of sharing limited to figures who were in fact marginal in the relevant context and unfortunately lacked the experience and appropriate tools that the circumstance would have required”
3.3.2. Need for discussion, training, and support. Concerning perceived support, most participants reported the need for regular discussions with colleagues about this issue (53%, n=8) and the hope for more education and training programs (20%, n=3), whereas five of them did not feel the necessity of further specific support.
“I feel the need for moments of free sharing but above all of participation and direct contribution from professional and guidance figures”
To the question Has anyone ever briefed you on what to do or how to cope with these events?, 14 out of 15 (93%) answered negatively.
4. DISCUSSION
To our knowledge, this is the first qualitative study on the impact of PS on psychiatric trainees and ECPs conducted in Italy. Based on the replies of 15 early career medical doctors involved in psychiatry working in an Italian university hospital, several different themes and sub-themes were identified. First, a significant emotional impact of PS was unveiled. Sadness and shock were the feelings most frequently reported by respondents. In particular, sadness was usually combined with other emotions ranging from inadequacy to anger. Feelings of guilt, impotence and inadequacy, disappointment, frustration, and anger were also broadly described. Second, PS reportedly had a strong influence on their subsequent clinical activity and approach. Indeed, PS seemed to encourage most of the trainees and ECPs surveyed to be more careful towards the patients’ needs and requests as well as to pay more attention to seemingly insignificant details. Along with this, the impression of being of limited help to the patient was commonly reported. Third, most of the surveyed subjects were seemingly able to share their emotional experience with peers. They also reported the need for regular discussions with colleagues about this issue, as well as the hope for more education and training programs, although to a lesser extent. However, the vast majority seems to have never been briefed on what to do or how to cope in the aftermath of this kind of event.
The thematic analysis approach used in our study favoured a general understanding of the feelings and needs of psychiatric trainees and ECPs after a PS, allowing us to analyse the emotional burden of such a frequent and dramatic event on this specific niche of young psychiatric trainees and ECPs, to identify its important consequences in the way they conduct their professional life and to intercept their needs.10
The findings from our study are in line with the existing literature on the topic30 in showing that experiencing PS poses a significant emotional burden on psychiatric trainees and ECPs. Although somewhat diverse across respondents, this set of unpleasant feelings highlights the fact that, not surprisingly, PS is a distressing circumstance that may affect young and unprepared professionals even more severely.13 Indeed, it has been suggested that the impact of PS is more significant when it occurs during training as compared with later stages of career, when relative defence mechanisms to this kind of events may develop.13 Amongst other factors, experiencing PS during early stages of career has been inversely correlated to clinicians’ perceived social integration into their network, a critical aspect in the first phases of their professional journey.15
PS seems to have a mixed influence on the subsequent clinical activity and approach of psychiatric trainees and ECPs, inducing them to be more attentive towards patients’ needs but also making them feel their hands are tied with respect to the real possibility of helping them, as also highlighted by the feelings of impotence, inadequacy, disappointment, and frustration which were largely reported. These themes, albeit indicating proactiveness and willingness to become better professionals on the one hand, denote a greater perceived responsibility for patients’ lives on the other. Added to this are fear, dejection for being afraid of not being up to par, and a generally reduced confidence both in their own clinical abilities and in the utility of psychiatric care. Increased engagement in clinical practice after a PS may come at the expense of heightened stress and discomfort. This effect is particularly pronounced in younger trainees when compared to more experienced colleagues.8,15,31,32 In line with the existing data, among the participants who had experienced a PS, we observed an increased tendency towards a more conservative approach when managing a patient at risk for suicide, with more proneness to hospitalize patients with suicide risk and an increased use of collegial consultation.33
In the aftermath of PS, there is no universally approved protocol available to support the psychiatrist who attended the deceased. However, experiences of medical professionals who have faced such distressing circumstances underscore several elements deemed invaluable or potentially advantageous.13,34 One crucial aspect is access to a senior clinician being able to understand the profound emotional impact of PS and offer confidential advice and support.13,34 Additionally, providing support to the formal processes that follow a PS can be instrumental. Clear guidance and assistance in navigating the administrative aspects can partially alleviate the burden.13,34 Moreover, there is a recognized need for a confidential reflective practice group or a designated space where psychiatrists can openly process the emotional effects stemming from the deaths of patients by suicide.13,34 Sharing experiences in a safe and confidential environment fosters a sense of community and understanding.13,34 Finally, individualised support also consists of one-to-one review of the conditions under which PS occurred.13,34 This personalised approach acknowledges the unique challenges each psychiatrist may face in the aftermath of such a tragic event.13,34 In essence, recognizing the sensitive nature of these situations and providing these supportive elements can contribute significantly to helping psychiatrists cope with the complexity of PS aftermath.13,34 In our sample, support from colleagues seemed particularly helpful, confirming findings in the literature. Notably, this kind of peer support was valued, as mentioned above.13 However, on the other hand, although the participants were informally offered the possibility to seek help from senior consultants from their own workplace, there was a lack of professional, structured support including the unavailability of contacts and of specific resources and systematic interventions, such as Balint groups or other structured groups. Subsequently, the hope for relevant interventions and programs was highlighted by most respondents. In sum, despite having appreciated the possibility of sharing emotions and feelings, managing “postvention” through a structured coping training seems to remain an unmet need, consistently with previous studies similarly observing that professionals who had experienced PS often feel that they have not received adequate training on this specific issue.33 It has been highlighted that professional reviews provide opportunities for learning and improved management of PS and its aftermath.7 Thus, more attention should be dedicated to preparing trainees and ECPs for this “occupational hazard” and to systematically implementing plans to support those who are especially vulnerable to the burden posed by PS.15
Both formal and informal networks should stimulate the recognition of the impact of PS on young and rather inexperienced professionals and take adequate measures to support them.15 As importantly, the responses to this survey may also suggest the need for greater social awareness around this delicate issue.15
4.1. Strengths and limitations
This work benefited from a qualitative approach, which enables us to appreciate nuances that we would not have grasped distributing a quantitative survey. Moreover, choosing a thematic analysis method with a semantic approach, which permits to identify themes at face value, ensured that the influence of investigators’ background and assumptions on the interpretation of data was as limited as possible. In addition, we did not collect information that could affect anonymity, minimising the risk of respondents to be recognized and thus allowing them to freely express themselves, their emotions, and their perspectives.
On the other hand, our findings should be interpreted with caution considering some methodological limitations. First, this was a single-site investigation, limiting the representativeness of our results. Second, the sample was small and homogenous in terms of age and experience. Both these issues might have led to the underestimation of some feelings and needs, possibly limiting the generalizability of our findings to other groups and professional figures. Third, although online surveys with an open-ended pattern have been extensively used for qualitative data collection, the use of an online tool may be limiting as compared to other possible data collection methods such as in-person interviews. Moreover, we cannot exclude that some questions may have been somewhat orienting. Lastly, we could not investigate how close each professional was to the patient in terms of therapeutic relationship, thus not making it possible to study how much this influenced participants’ replies. Since a “continuum of survivorship” has been identified distinguishing those who are bereaved by, affected by, or exposed to a suicide, with different effects depending on the professional role and the type of bond built with the patient,35 this is surely an aspect that deserves to be taken into account in future investigations.
5. CONCLUSIONS
Our findings add to the existing evidence supporting the importance of addressing the strong emotional effect of PS on psychiatric trainees and ECPs as well as the necessity for more structured support strategies in the aftermath of such a dramatic event. In view of the met and unmet needs highlighted by our study, we hope that training programs are implemented in this direction in order to allow early career professionals in the field of mental health care to be better prepared for an eventual PS as well as to help them cope with it afterwards. Larger and multi-centre investigations are warranted to investigate the influence of PS on the personal and professional life of psychiatric trainees and ECPs more in depth.
Declarations of Interest
Daniele Cavaleri is an Editorial Board member of the International Journal of Psychiatric Trainees. He has signed a non-interference statement and has resigned from any involvement in the editorial process of this article.
Funding Source Declaration
This research received no specific grant from any funding agency in the public, commercial or not-for-profit sectors.
Author contributions
GL, MDV, DC, and SIP Giovani designed the study. GL wrote the survey questions and collected the data. GL, MDV, and DC analysed the data. GL, MDV, and DC wrote the first draft of the manuscript. SIP Giovani supervised the entire work and revised the first and subsequent drafts of the manuscript.
Author Agreement
All authors have approved the final version of the manuscript.
Coordinamento Nazionale Giovani Psichiatri of Società Italiana di Psichiatria (“SIP Giovani”) Claudia Palumbo, Gaia Sampogna (National Coordinators); Mariangela Corbo, Giacomo D’Andrea, Mauro Pettorruso (Regional Coordinators for Abruzzo and Molise); Renato De Filippis (Regional Coordinator for Calabria); Luigi Giuliani (Regional Coordinator for Campania); Corinna Reggianini, Rosa Sant’Angelo (Regional Coordinators for Emilia-Romagna); Ilaria Adulti, Delfina Janiri (Regional Coordinators for Lazio); Davide Prestia (Regional Coordinator for Liguria); Simone Cavallotti, Matteo Rocchetti (Regional Coordinators for Lombardy); Federico Biondini, Laura Orsolini, Simone Pompili (Regional Coordinators for Marche); Luigi Girardi (Regional Coordinator for Piedmont); Gianluigi Caputo, Francesco Piarulli (Regional Coordinators for Apulia and Basilicata); Lucia Sanna, Sara Piras (Regional Coordinator for Sardinia); Roberta Arcoleo, Alessandro Rodolico (Regional Coordinators for Sicily); Carlo Bertelloni (Regional Coordinator for Tuscany); Carlotta Ficco (Regional Coordinator for Trentino-South Tyrol); Giulia Menculini (Regional Coordinator for Umbria); Carla Comacchio, Michele Raffaelli (Regional Coordinators for Veneto)."
Acknowledgements
None.